 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
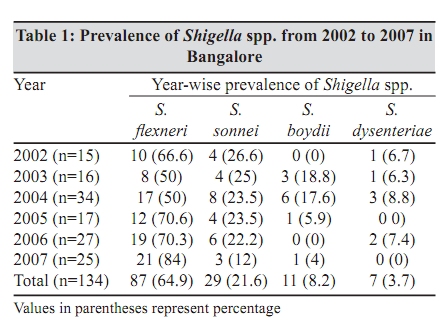
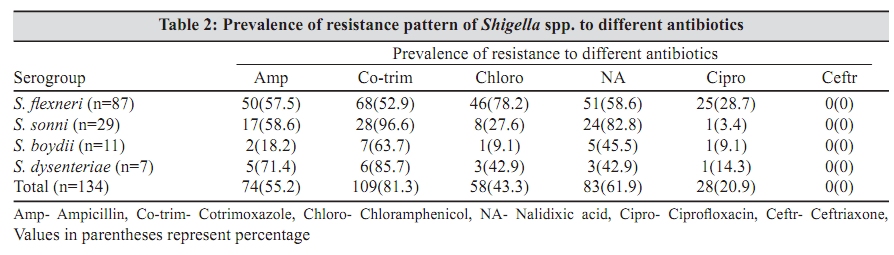
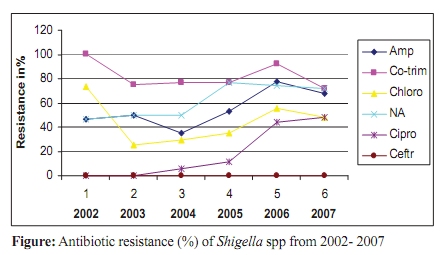
Indian Journal of Medical Microbiology, Vol. 27, No. 4, October-December, 2009, pp. 358-360 Brief Communication Magnitude of drug resistant shigellosis: A report from Bangalore H Srinivasa, *M Baijayanti, Y Raksha Department of Microbiology, St. John's Medical College, Bangalore - 560 034, India Correspondence Address: *Department of Microbiology, St. John's Medical College, Bangalore - 560 034, India, baijayantimishra@gmail.com Date of Submission: 14-Oct-2008 Code Number: mb0999 PMID: 19736408 DOI: 10.4103/0255-0857.55460 Abstract Shigella is an important cause of acute invasive diarrhea in children and others. Antimicrobial susceptibility of Shigella spp. isolated from diarrhoeal/ dysenteric patients in Bangalore was studied in our hospital from January 2002 to December 2007. One hundred and thirty-four isolates were identified as Shigella species. S. flexneri, S. sonnei , S. boydii and S. dysenteriae were accounted respectively for 64.9%, 21.6%, 8.2% and 3.7% of the total number of Shigella isolated. Of these 56 (41.8%) were from children (0 to 14 years) and 78 (58.2%) were from adults and elderly patients. Over 70% of Shigella isolates were resistant to two or more drugs including Ampicillin and Co-trimoxazole. During 2002 to 2007, resistance to Ampicillin had increased from 46.7% to 68%. For Co-trimoxazole, though the resistance had gradually decreased from 100% to 72%, but still the resistance is high. Chloramphenicol resistance showed sudden decline from 73.3% to 25% from 2002 to 2003, but gradually has reached 48%. Nalidixic acid resistance was more than 70%. All isolates were sensitive to Ciprofloxacin during the period 2002 to 2004, but over the years the resistance pattern gradually increased up to 48%. Ceftriaxone had shown no resistance. The results of the study revealed the endemicity of Shigellosis with S. flexneri as the predominant serogroup. Children were at a higher risk of severe shigellosis. The results also suggest that Ampicillin, Co-trimoxazole, Chloramphenicol, Nalidixic acid and Ciprofloxacin should not be used empirically as the first line drugs in the treatment of Shigellosis. Periodic analysis and reporting of antibiotic susceptibility is an important measure to guide antibiotic treatment.Keywords: Antibiotic resistance, Bangalore, dysentery/diarrhea, Shigella Introduction Shigellosis still remains a public health problem in most developing countries because of the poverty, poor sanitation, personal hygiene and poor water supply. [1] Literature review shows that about 140 million people suffer from shigellosis with estimated 600,000 deaths per year world-wide. [2],[3] It is a major cause of dysentery/diarrhea in children and others. Many of them are hospitalized immediately after the onset of the disease. Though, oral rehydration is the principal means of management, because of the enteroinvasiveness antibacterial treatment may be necessary. [1] The number of multiresistant strains are increasing regularly not only in different parts of the country, but also world-wide. [1],[2],[3],[4],[5],[6],[7],[8] Hence the study was carried out to determine the antibiotic susceptibility profile of Shigella spp. in Bangalore. Materials and Methods During January 2002 to December 2007, 2941 stool samples were collected from diarrhoeal/dysenteric patients admitted to the hospital. The patients included children, adults and elderly people. Fresh faeces of patients were collected and transported immediately for culture. The specimens were inoculated on MacConkey agar, Salmonella- Shigella agar, Xylose-Lysine deoxycholate media and Selenite-F enrichment broth. [9] Suspected Colonies of Shigella were subjected to standard biochemical tests using Triple sugar iron agar, Mannitol motility medium, Indole production and Lysine iron agar medium. Specific anti-sera (Denken-Seika, Japan Shigella antisera) were used for serotyping of isolated Shigella . The susceptibility of all the isolated Shigella to different antibiotics were determined by Kirby-Bauer's disk diffusion technique as per the CLSI guidelines. [10] The antibiotics used were Ampicillin, Co-trimoxazole, Chloramphenicol, Nalidixic acid, Ciprofloxacin and Ceftriaxone. Results Of the 2,941 diarrhoeal/dysenteric stool samples screened, Shigella strains were identified in 134 (4.6%) samples. Shigella spp. were isolated from patients with ages ranging between 0 to> 70 years. Of these, 56 (41.8%) were from children from 0 to 14 years and the rest 78 (58.2%) were from adults and elderly patients. The clinical course was found to be more severe in children with superadded malnutrition. Males out-numbered the females in all the age groups . S. flexneri strains were identified in 84 (64.9%) Shigella positive cultures, while S. sonnei accounted for 29 (21.6%). S. boydii was isolated in 11 (8.2%) and S. dysenteriae in 5 (3.7%) of the total number of isolates [Table - 1]. S. flexneri has been the predominant isolate during the period of the study. However the percentage dropped in 2003 and 2004 from an average of 70% to 50%. During this period S. boydii has increased to about 18%. [Table - 1]. The prevalence of resistance pattern of Shigella spp. isolated between 2002 to 2007 is as shown in [Table - 2]. Over 70% of Shigella, isolates were resistant to two or more drugs including Ampicillin and Co-trimoxazole. Resistance rate of Ampicillin was 55.2%, Co-trimoxazole 81.3%, Chloramphenicol 43.3%, Nalidixic acid 61.9% and Ciprofloxacin 20.9%. No resistance was observed to ceftriaxone during the study period. Considering prevalence of resistance pattern in different serogroups, S. flexneri showed highest resistance to Chloramphenicol (52.9%) and Ciprofloxacin (28.7%), S. sonnei to Nalidixic acid (82.8%) and Co-trimoxazole (96.6%) and S. dysenteriae to Ampicillin (71.4%) [Table - 2]. Year-wise resistance pattern in Shigella spp. is shown in [Figure - 1]. Discussion Shigellosis is endemic in our region as evidenced by the continued isolation of Shigella over the 5 year period. In this study, we isolated 134(5.4%) Shigella strains from diarrhoeal/dysenteric stools of 2491 patients. The percentage over 5 years varied between 2.8% to 5.9%. This was similar to the Vellore data, 3.9% in 2001. [4] The pattern of Shigellosis indicates that S. flexneri was the predominant and most active serogroup in Bangalore during the years. The numbers of faecal samples submitted to the laboratory were more or less similar in all the 5 years, but in 2004 more Shigella were isolated (5.9%). This increase in isolation of Shigella seems to be real and not due to increased number of stool cultures during that period. A minor outbreak could be the reason behind the increase. The pattern of Shigellosis indicates that S. flexneri was the predominant and most active serogroup in Bangalore during the years. However, in 2003 and 2004, S. boydii was isolated from 18% of cases reducing S. flexneri from near 70% to 50%. In 2007, S. sonnei had been reduced by 10% and the isolation rate of S . flexneri increased from 70% to 80% [Table - 1]. This cyclic change agrees with the pattern observed in Puducherry and Kolkata where cyclical serogroup change had been observed over the years. [6],[8] Analysis by age showed that 56 (41.8%) were from pediatric age group (0-14 years). The clinical course was found to be more severe in children superadded with malnutrition. This calls for an urgent measure to reduce the deaths in children due to Shigellosis. Therefore, public health strategy should ensure clean water supply, good sewage management and a clean environment. Analysis of the antibiotic susceptibility data showed a gradual increase in resistance to Ampicillin, fluctuating resistance to Chloramphenicol and persistent resistance to Co-trimoxazole. Over 70% of Shigella isolates were resistant to two or more drugs including Ampicillin and Co-trimoxazole. Similar findings were reported from Manipal, South India by Mamata et al . [7] and overall 90% were reported from Kolkata by Niyogi et al . [5] In our study, there is a gradual increase in Ampicillin resistance, 46.7% to 68% from 2002 to 2007. Similar findings have been seen in Puducherry where resistance was 46% in 2005, 57% in 2006 and 55% in 2007. Co-trimoxazole resistance decreased from 100% in 2002 to 72% in 2007, but still high enough to discourage empiric use. Similarly Chloramphenicol resistance decreased from 73.3% in 2002 to 25% in 2003 and gradually increased to 48% in 2007. Resistance to Nalidixic acid increased from 46.7% in 2002 to 72% in 2007. Ampicillin, Co-trimoxazole, Nalidixic acid and Chloramphenicol were considered as first line antibiotics for treatment of Shigellosis empirically, but it is no longer true. Nalidixic acid resistance had emerged in 2002 and steadily increased from 2003 to 2007. Similar high rate of resistance was reported in Vellore and Kolkata. [4],[5] Flouroquinolone resistance was noted in 2004 (5.9%) and gradually increased to 48.5% in 2007. A similar trend of increased Ciprofloxacin resistance has been observed in other parts of India. [6],[8] The molecular characterization of 60 strains has been done by Gururaj et al . between 2001 and 2004. [11] Their findings showed that Flouroquinolone resistant strains had a uniform mutation in Gyr-A at position 83 (replacement of serine with leucine and the majority of strains had a second mutation at position 87 with replacement of aspartic acid with either glycine or aspargine. The clinical course though was more severe in Ciprofloxacin resistant cases, no mortality was observed in our study. These patients were treated symptomatically as well as with a third generation Cephalosporin. The emergence of Flouroquinolone resistant Shigella has a bearing on therapy of Shigellosis as many clinicians empirically prescribe Flouroquinolones for many infections like diarrhea and urinary tract infection. Thus with the emergence of high resistance there is a need for alternate drugs. Most of the isolates were susceptible to Neomycin and Furazolidine. All were susceptible to Ceftriaxone. This was similar to the study by Mamatha et al . at Manipal. [7] Recently however in January 2009 we have isolated a strain of S. flexneri resistant to Ceftriaxone with MIC 64µg/ml (confirmed by Vitek 2C), simultaneously resistant to Ampicillin, Co-trimoxazole, Chloramphenicol, Nalidixic acid, Ciprofloxacin and Furazolidine. Though the patient was managed symptomatically, spread of the clone may pose a greater threat to the community. More data are required from different parts of the country to support our finding. Data from the literature suggest that Azithromycin and Mecillinam have shown promise in treatment of Shigellosis. [12],[13] The study shows the occurrence of drug resistant Shigellosis. Antibiotics may not be necessary for mild cases and if required should be guided by local data. The continuous surveillance of multidrug resistant strains is very important to know the changing antibiotic susceptibility pattern as well as the cyclical change of the serogroup from time to time as the resistance pattern also changes with the change in the serogroup. Analysis and periodic reporting is important in proper therapy of Shigellosis. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09099t1.jpg] [mb09099f1.jpg] [mb09099t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}