 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
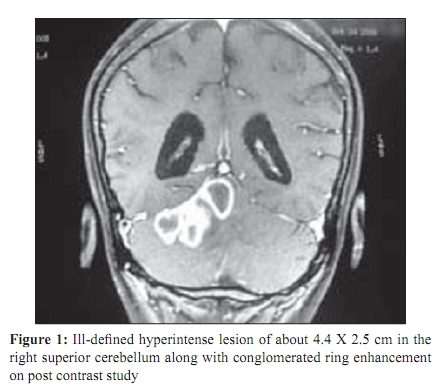
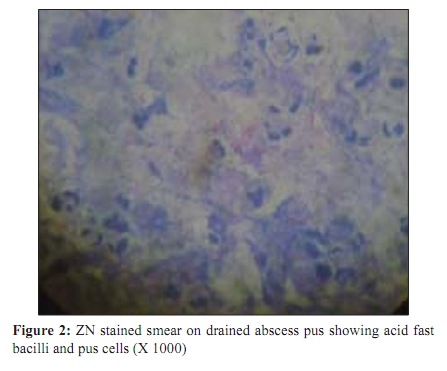
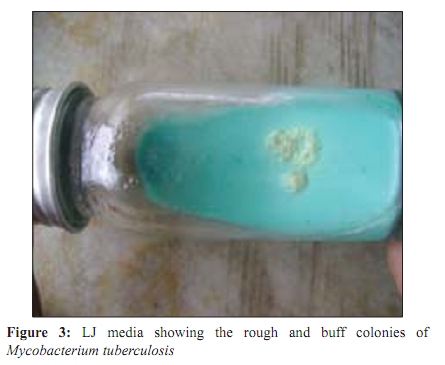
Indian Journal of Medical Microbiology, Vol. 27, No. 4, October-December, 2009, pp. 363-365 Case Report A rare case of tubercular cerebellar abscess K Wanjari, *VP Baradkar, G Nataraj, S Kumar Department of Microbiology, Lokmanya Tilak Municipal Medical College General Hospital, Sion - 400 022, Mumbai, India Correspondence Address: *Department of Microbiology, Lokmanya Tilak Municipal Medical College General Hospital, Sion - 400 022, Mumbai, India, vasantbaradkar@yahoo.com Date of Submission: 30-Dec-2008 Code Number: mb09101 PMID: 19736410 DOI: 10.4103/0255-0857.55464 Abstract Tubercular brain abscess are uncommon and tubercular cerebellar abscess are rarely reported. Most of these cases occur in immunocompromised patients. We report a case of multiple cerebellar abscesses in a 55-year-old HIV seronegative non-diabetic female, who complained of headache, neck pain and unsteadiness of gait since two months. She had been on treatment for pulmonary tuberculosis, diagnosed earlier. Diagnosis was made by CT scan of brain and confirmed by bacteriological examination of drained pus obtained by suboccipital craniotomy. The patient showed signs of recovery.Keywords: Cerebellar abscess, tubercular abscess Introduction Extrapulmonary tuberculosis is observed in approximately 20% of all tuberculosis (TB) cases and its incidence has increased in the recent years. [1],[2],[3] Central nervous system (CNS) tuberculosis, the most dangerous form of tuberculosis, accounts for approximately 5% of extrapulmonary tuberculosis. Tuberculous meningitis (TBM) is the most common form of CNS- TB; however solitary or multiple intracranial tuberculomas, in particular occur less frequently. [1],[2],[3],[4],[5] In the differential diagnosis of intra-cranial tuberculosis (ICTS), images on the radiological findings should be differentiated from other causes of space occupying lesions, which include malignant diseases such as glioma or lymphoma, pyogenic abscess, toxoplasmosis, neurocysticercosis, sarcoidosis, hydatidosis and late syphilitic involvement of CNS. [1] The initial diagnosis is based on radiological findings, but definitive diagnosis is done by bacteriological methods. We report a case of multiple cerebellar abscesses in a 55-year-old female. The initial diagnosis of tubercular abscess was confirmed by the isolation of Mycobacterium tuberculosis from drained abscess material. Case Report A 55-year-old female patient complained of headache, neck pain and unsteadiness of gait for two months. The patient, on treatment for pulmonary tuberculosis, diagnosed six months earlier, was non-diabetic and non-hypertensive. The fundus examination showed bilateral papilledema. There were no signs suggestive of cranial nerve palsy. Her pulse rate was 76/min, the blood pressure was 130/80mm Hg, jugular venous pressure was not raised and the precordial activity was normal. The respiratory and cardiovascular systems were within normal limits. The patient was seronegative for HIV antibodies. Her hemoglobin was 10gm/dl, total leukocyte count was 18,000/mm 3 , with 80% neutrophils and 20% lymphocytes. The ESR was slightly raised at 40/hour. Her renal and liver function tests were within normal limits. The CSF findings showed 50 lymphocytes/mm 3 and the proteins were 100mg/dl. Xray of the chest showed features of bilateral pulmonary tuberculosis with multiple patchy consolidations. Computerised Tomography (CT Scan) findings of CNS showed multiple abscesses at the cerebello-pontine angle [Figure - 1]. In the right superior cerebellum, ill-defined hyperintense lesions of about 4.4 X 2.5 cm were noted. Conglomerated ring enhancement on post contrast study was noted, and mild perilesional edema was seen. The mass resulted in compression over the adjacent cerebellar parenchyma and dorsal brain stem. A small ring enhancing lesion was also seen in the right temporo-occipital region. The fourth ventricle was effaced while rest of the ventricles were prominent. The sulci and cisterns were unremarkable. No significant shift of midline structures was observed. The findings revealed conglomerated ring enhancing lesions in the right cerebellum and right temporo-occipital region, suggestive of tubercular abscess. Suboccipital craniotomy was done and the abscess was drained. The Gram stained smear of the pus cells showed pus cells, with no organisms, while the Ziehl Neelsen staining revealed acid fast bacilli and pus cells [Figure - 2]. The sample was inoculated on Blood agar, Chocolate agar, Thioglycollate broth and Lowenstein- Jensen medium. No growth was observed on Blood agar, Chocolate agar plates and even after prolonged incubation for six weeks there was no growth observed in the Thioglycollate medium. The histopathological examination showed inflammatory cells but there was no evidence of Langhan's giant cells or caseation. Culture on Lowenstein Jensen media showed rough and buff colonies suggestive of Mycobacterium tuberculosis [Figure - 3] after four weeks of incubation and was confirmed by acid fast staining (with 25% sulfuric acid as a decloriser), and biochemical tests. The patient, meanwhile, was started on Category II regimen of DOTS. She responded well to the drainage of the abscess and the anti-tubercular regimen, and was later discharged after a period of four weeks, without any residual neurological deficit. At a four month follow up, the patient was doing well on the regimen and the repeat Xray, showed signs of resolution of symptoms and three early morning samples for acid-fast bacilli were negative. Discussion The organisms most frequently isolated from brain abscesses are Staphylococcus aureus , Gram-negative bacilli, anaerobes and Streptococcus viridans . [1],[2],[3] Tubercular brain abscess is rather rare in places where tuberculosis is endemic, like India. Intracranial tuberculoma may compromise as many as 10% of all intracerebral space occupying lesions (ICSOL). [4] This figure may touch more than 20% in children. Cerebral tuberculosis manifests predominantly as tuberculous meninigitis, [1],[2],[3],[4],[5] followed by tuberculomas, other forms of CNS tuberculosis include cerebral abscess, cerebral miliary tuberculosis, tuberculous encephalopathy, tuberculous encephalitis and tuberculous arteritis. Tuberculous abscess of the brain are very uncommon and that too cerebral abscess is very rare. Reddy GN & Prusiy [5] reviewed 206 cases of intracranial tuberculomas operated at the National Institute of Mental Health Neurosciences, Bangalore between 1959-1980. All these cases were analysed retrospectively. Four different types of presentations observed included tuberculoma with grape like multiple arachnoid cysts, tuberculous abscesses of cerebellum with concomitant tuberculous meningitis, tuberculoma presenting to a psychiatrist and chronic tuberculoma of more than five years duration. Gazzaz et al . [6] reported tubercular cerebral abscess in the year 2000, which responded with surgical and antitubercular treatment. Recently, Ramesh VG & Sunder KS [2] reported a case of concomitant tuberculosis and pyogenic cerebellar abscess in patients with pulmonary tuberculosis, who responded to suboccipital craniotomy, antitubercular treatment and antibiotics. The patient came with similar complaints i.e. neck pain, unsteadiness of gait as observed in this case. Though tuberculosis in CNS occurs due to hematogenous spread of Mycobacteria from elsewhere; TBM may occur via lymphatic spread from cervical lymph nodes. Tubercle bacilli are immobilized in end-arteries, which leads to formation of submeningeal tubercular foci, which may further lead to various presentations of tuberculosis [4] . In tuberculoma, bacilli get lodged in brain with rich blood supply. Once tuberculoma is formed, it evokes secondary reaction, leading to capsule formation. The surrounding brain edema and gliosis may resemble low-grade astrocytoma. In rare cases, there may be central caseation, liquefaction and formation of an abscess. This phenomenon is very rare, tuberculous abscess commonly occurs in patients with abnormal cell mediated immunity and are mostly focal. [4],[5] These lesions are usually secondary to lung disease, as observed in the present case and at the junction of gray and white matter. Histologically and clinically these abscesses are similar to pyogenic abscesses. Tuberculous abscess is devoid of granulomatous reaction associated with tuberculosis. The criteria for diagnosis include pus within brain, bacteriological proof or histological confirmation of the abscess. All these criteria were met during diagnosis of cerebellar abscess in the present case report. The presentation is reported mostly in 3 rd or 4 th decade. There may be supratentorial abscess and rarely in cerebellum as observed in the present case. [1],[2],[3],[4],[5] As bacteriological diagnosis is the best proof of CNS tuberculosis, any cerebral manifestation in a known case of pulmonary tuberculosis should be investigated properly for early diagnosis and treatment. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09101f3.jpg] [mb09101f2.jpg] [mb09101f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}