 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
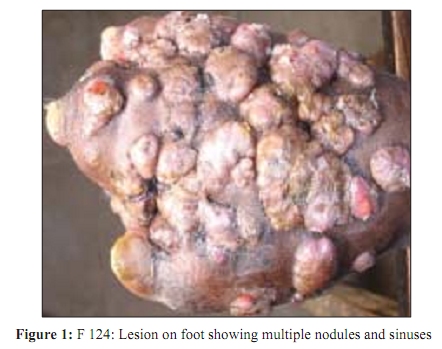
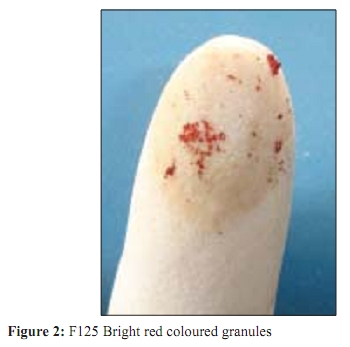
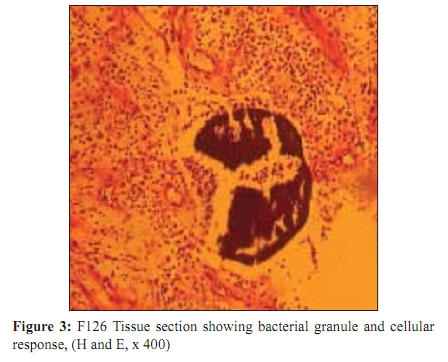
Indian Journal of Medical Microbiology, Vol. 27, No. 4, October-December, 2009, pp. 370-372 Case Report Red grain botryomycosis due to Staphylococcus aureus - A novel case report *V Katkar, F Mohammad, S Raut, R Amir Department of Microbiology (VK, FM, SR), Skin and V. D (RA), Government Medical College, Nagpur 440 003, India Correspondence Address: *Department of Microbiology (VK, FM, SR), Skin and V. D (RA), Government Medical College, Nagpur 440 003, India, vyankateshkatkar@yahoomail.com Date of Submission: 05-Apr-2009 Code Number: mb09104 PMID: 19736413 DOI: 10.4103/0255-0857.55458 Abstract Staphylococcus aureus and some other bacteria are known to cause botryomycosis. These bacteria are known to produce yellowish-white soft grains. Only Actinomadura pelletieri is known to produce red grains. We report here a case of an intensely inflammatory type of botryomycosis. A 35-year-old male labourer presented with swelling, redness and multiple sinuses on his foot, of eight months duration. The purulent discharge contained bright red coloured grains, 0.5 to 1 mm in size, which were round to oval in shape. Gram-positive cocci were demonstrated in crushed granules and tissue sections. Culture yielded pure and heavy growth of Staphylococcus aureus . He responded very well to cefazolin. There is no other report of such red grain botryomycosis due to Staphylococcus aureus , available in literature. This is first case report of its kind in world literature.Keywords: Botryomycosis, red grain, Staphylococcus aureus Introduction Botryomycosis is characterized by chronic, purulent and granulomatous lesions of the dermis, and subdermal tissue and viscera. Similar to eumycetoma and actinomycetoma, it is characterized by tumefaction, sinus tract formation and discharge of sulphur granules. Staphylococcus aureus and Staphylococcus epidermidis are the most common agents, but other species like Pseudomonas aeruginosa, Escherichia coli, Proteus, Bacteroides and some other bacteria are fairly common. [1] Hands, pinna, feet and head are common sites of botryomycosis, although any part of the body skin may be involved. Folds of skin in obese persons, skin under pendulous breasts are other vulnerable areas. [1] Botryomycosis can be cutaneous or visceral. Visceral botryomycosis may be a primary or a secondary infection due to dissemination. Pulmonary botryomycosis is the most common entity in visceral involvement. [1],[2],[3] Intraoral granulomatous pyogenic botryomycosis has also been reported. [4] Surgery, abrasions and lacerations in road accidents, piercing of pinna are documented etiological factors that may lead to the development of botryomycosis. Chronic cutaneous irritation and lichenified lesions of the scalp often predispose to botryomycosis. Diabetes, alcoholism, poor hygiene, cystic fibrosis and general debility are the known predisposing factors. Botryomycosis is often associated with children. In most cases infection remains localized, although occasionally it spreads to other organs like the liver, kidney, lungs, heart and prostate, and lymph nodes may occur. [1] It is increasingly being reported from AIDS cases. [3] Cellular response in general is similar to actinomycetoma and eumycetoma. The grain is surrounded by acute suppurative response. Neutrophils in various stages of degeneration, in large numbers, are seen surrounding the grain. Lymphocytes, eosinophils, plasma cells, histiocytes, few foreign body giant cells and fibroblasts surround the central suppuration; Surrounding this is the fibrosis and granulation response, with capillary formation. [1] Case Report A 35-year-old male labourer presented with swelling, redness and multiple sinuses, with foul smelling discharge containing red granules. He gave a history of trauma on the foot, with an iron rod, eight months back. In a few days, he noticed a small nodule, on the back of right foot. Gradually the swelling increased in size, and formed a discharging sinus. In the following months many more nodules and sinuses appeared around this lesion. On examination, it was observed that the entire back of the right foot was severely swollen with intense erythema, with numerous elevated, well-demarcated, small and large nodular lesions and many discharging sinuses were present [Figure - 1]. Sinus openings were inflamed and mostly blocked with dried pus and sulphur granules. The foot appeared grossly deformed, and it was tender. Veins of the right leg were dilated and pitting edema extended almost up to the knee. Discharge was yellowish, purulent, foul smelling and contained abundant fine red granules. The red granules were easily visible on the undersurface of the dressing as well. Pus was collected in a sterile bottle by aspirating with a sterile Pasteur pipette. Plenty of fine sandy bright red coloured grains were visible in the pus [Figure - 2]. A piece of biopsy 4 x 6 mm was obtained from one of the nodular swellings and subjected to a histopathological examination. A thorough physical examination revealed no other abnormality except that the patient had mild fever and a pulse rate of 90/minute, haemoglobin was 10 gm/dl; total leukocyte count was 12000/mm 3 , and polymorph count was 84%. He was non-reactive for HIV and there was no evidence of any other disease or abnormality. In the laboratory the pus was transferred to a sterile Petri dish. Few red grains were picked up with a sterile blunt forceps and transferred to a drop of sterile saline in another petri dish. Any loose matter sticking to the surface was removed with a teasing needle and transferred to a fresh drop of saline five times, to complete the washing process. On examination the grains were found to be 0.5 to 1 mm in size and round to oval in shape with fairly regular margins. Two grains were crushed between two sterile glass slides. One of the slides was used for Gram staining and wet mount preparation and the other for culture. The grains were soft, and could be easily crushed between two slides. A Gram-stained smear of the crushed granule revealed a compact, granular, gram-positive mass, made of Gram-positive spherical cocci, which were about 1 µ in size. Wet mount did not show any fungal element. Culture was done on a sheep blood agar plate at 37 0 C and Sabouraud Dextrose Agar (SDA) with antibiotics at room temperature and at 37 0 C. One slant of Lowenstein-Jensen (LJ) was inoculated and observed for eight weeks. Culture on blood agar yielded pure and heavy growth of golden yellow, beta hemolytic colonies after overnight incubation. Gram stain, positive catalase test, mannitol fermentation and positive slide and tube coagulase test confirmed it to be Staphylococcus aureus. It was sensitive to oxacillin and cefazolin, but resistant to penicillin, gentamicin and ciprofloxacin. No growth was obtained on either SDA or LJ slants. Histopathology of the biopsy showed many granulomatous foci. Grains were compact and round to oval, with regular margins and granular appearance, and were present at the center of the granuloma. The granules were surrounded by neutrophils, lymphocytes, histiocytes, fibroblasts and an occasional plasma cell or foreign body giant cell. The outer zone showed granulation tissue. The granules contained a compact mass of basophilic cocci embedded in a eosinophilic matrix [Figure - 3]. The patient responded well to cefazolin with significant reduction in the swelling, stoppage of discharge and disappearance of fever within 13 days of observed treatment. The patient was discharged against medical advice and did not come for follow up Discussion Staphylococcus aureus is a well-recognized agent of botryomycosis. [1],[2] Staphylococcus aureus and other bacteria are known to produce white grain botryomycosis. The grains are usually round to oval in shape, up to 1 mm in size, yellowish white in colour and are composed of a bacterial mass embedded in a eosinophilic matrix. This is the first case report of red grain botryomycosis. Although in this case the grains were intensely red, the colour of the colonies was golden yellow. The etiological role of Staphylococcus aureus is supported by the following observations: (a) the microscopy of the grains showed a presence of gram-positive spherical cocci, (b) there was discharge of grains in abundance, (c) the grains yielded heavy and pure growth of beta hemolytic, golden yellow colonies of Staphylococcus aureus , which were coagulase positive, (d) in the tissue sections sulphur granules composed of gram-positive coccal masses were observed and the cellular response was in line with that of botryomycosis, (e) there was no evidence of any other pathogen in the grain, pus or tissue samples in microscopy or culture, and (f) the patient responded quite well to cefazolin treatment. A cell-mediated immuity (CMI) defect leading to atypical tissue response and reduced phagocytosis has been postulated as an important factor in the pathogenesis of botryomycosis. In the present case, the tissue section is in agreement with this fact, as not much of the phagocytosis of Staphylococcus is evident. Only Actinomadura pelletieri is known to produce red coloured grains. [1],[5],[6] We could not find any report of red coloured grain production by Staphylococcus species or any other bacteria for that matter. Hence we consider this as the first report, in world literature, on the production of red grain botryomycosis by Staphylococcus aureus. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09104f3.jpg] [mb09104f1.jpg] [mb09104f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}