 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
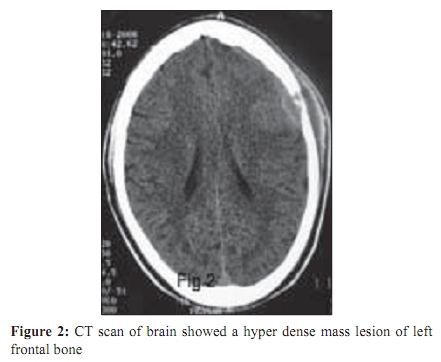
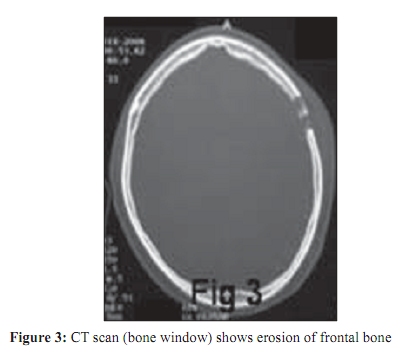
Indian Journal of Medical Microbiology, Vol. 27, No. 4, October-December, 2009, pp. 380-381 Correspondence Calvarial tubercular osteomyelitic abscess *A Rajesh1 , AK Purohit1 , V Lakshmi2 Departments of Neurosurgery (AR, AKP), Microbiology (VL), Nizams Institute of Medical Sciences, Hyderabad - 500 082, India Correspondence Address:Department of Neurosurgery, Nizams Institute of Medical Sciences, Hyderabad - 500 082, India, drarajesh1306@gmail.com Date of Submission: 04-Feb-2009 Code Number: mb09111 PMID: 19736420 DOI: 10.4103/0255-0857.55444 Dear Editor, Tuberculosis which is quite common in developing countries is on an upsurge in developed countries in association with immune deficiency syndromes. Reid in 1842, described the first case of calvarial tuberculosis. [1] Raut et al ., reported in their study for a decade, 42 cases of calvarial tuberculosis confirming the rarity of tuberculous lesion in skull. [2] This 29 year-old male, presented to us in April, 2008, with headache and scalp swelling over the left frontal region, treated with over the counter analgesics. The progressive increase in size of the swelling and non-remitting pain brought the patient to us. No history of trauma noted. The patient was afebrile on examination. Examination of the scalp showed a solitary, erythematous, slightly tender, fluctuant, non-pulsatile, non-mobile swelling of size 4 cm diameter. Laboratory investigations showed Hb - 12.6 g%, TLC - 5,000/mm 3 , DC - N70, L23, E4, M3, ESR- 24mm/hr, Mantoux - 20mm at 72 hours. Routine biochemical parameters were normal. Chest radiograph posterior-anterior view was normal [Figure - 1]. A CT scan of brain showed a hyperdense mass lesion of left frontal bone [Figure - 2],[Figure - 3] of size 3.5cm x 2cm x 2cm located 0.5 cm anterior to left coronal suture, with erosion of both inner and outer tables of the skull and sub-galeal collection. Left fronto-temporal curvilinear incision and evacuation of pus, debridement of granulation tissue and removal of involved bone was performed. Histopathology showed granulomatous lesion with epitheloid cells. The pus was sent for Gram's staining, fungal staining, acid fast staining, aerobic, fungal and mycobacterial culture, for evaluation of abscesses alongwith histological examination. All the staining reports were negative and we could only grow mycobacterium in culture. The patient was screened for HIV/ HBsAg/ HCV and routine hematological examination as per hospital protocol for pre-operative assessment which were within normal limits. Routine urine microscopy was normal. The patient had no history suggestive of immune disorders/ high risk behavior. No additional tests for immunological status assessment were performed considering a reactive Mantoux. Culture for Mycobacterium tuberculosis by BACTEC - 460 Tbsystem (Becton Dickinson, USA) using the 12 B vials, showed growth of M. tuberculosis at the end of 5 weeks. The patient was started on four drug anti-tubercular regime (INH, Rifampicin, Ethambutol and Pyrazinamide, as per RNTCP protocol). Follow-up after one month showed good healing of scar and repeat ESR was 12mm/hr. At a one year follow-up, the patient is doing well with no recurrence of the lesion. Tuberculous involvement of calvarium is rare as compared to other osseous involvement. The flat bones of skull contain little cancellous bone and hence rarity of the involvement of skull. However, in the skull itself, it occurs more commonly in the frontal and parietal bones [2] which have greater bone marrow than the occipital bone. Trauma [4],[5] and tuberculosis of other sites [3] may/may not be associated with skull tuberculosis. Surgical curettage followed by anti- tuberculous drug therapy is the treatment of choice, having good prognosis. Acknowledgment Scientific contribution of Dr. A. Praveen and Dr. I. Dinakar is gratefully acknowledged. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09111f2.jpg] [mb09111f3.jpg] [mb09111f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}