 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
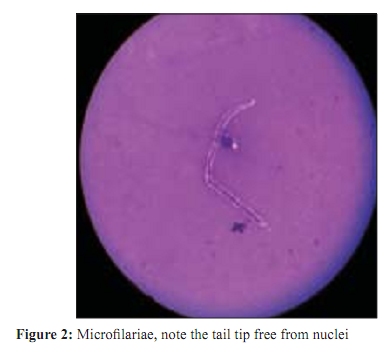
Indian Journal of Medical Microbiology, Vol. 27, No. 4, October-December, 2009, pp. 382-383 Correspondence An unusual presentation of Wuchereria bancrofti infection *V Rawat, G Rizvi, N Sharma, H Pandey Departments of Microbiology (VR), Pathology (GR, HR), Surgery (NS), UFHT, Medical College, Haldwani, Nainital - 263 129, India Correspondence Address: Department of Microbiology, UFHT, Medical College, Haldwani, Nainital - 263 129, India, drvinitarawt31@rediffmailcom Date of Submission: 07-Feb-2009 Code Number: mb09112 PMID: 19736421 DOI: 10.4103/0255-0857.55442 Dear Editor, Bancroftian filariasis is widely distributed throughout the tropics and sub-tropics. [1] Despite the large number of people affected, it is unusual to find microfilaria in routine cytological smear and their recognition is generally considered an incidental finding. [2] We describe a case of a 45-year-old woman presented with a firm indurated sub-cutaneous swelling measuring 4 x 2.5 cm on the flexor surface of right arm [Figure - 1]. Fine needle aspiration cytology (FNAC) of the swelling revealed straw colored fluid with large number of microfilariae on microscopic examination, identified as Wuchereria bancrofti because of the presence of hyaline sheath, cephalic space length: breath ratio was 1:1, nuclei were almost spherical, regularly placed, appeared in regular row, well separated without any overlapping and were absent at the tip tail [Figure - 2]. We could not find adult worm or its segment in aspiration material. Subsequent identification on smear, night blood smear from patient failed to demonstrate microfilariae and blood eosinophil counts were within normal range (2%). Serum was collected and sent for antibodies detection in JB Tropical Disease Research Centre Mahatma Gandhi Institute of Medical Sciences, Sevagram. Indirect ELISA was performed which was highly positive for specific recombinant Wuchereria bancrofti filarial antigen (WL-L2). Swelling subsided after administration of diethylcarbamazine (100mg TDS) for 21 days. Diagnosis of filarial infection is frequently made on strict clinical ground in endemic areas, but demonstration of microfilariae in circulating blood is the only means by which one can make definite diagnosis. [2] Similar to our finding, subsequent peripheral examination following cytological diagnosis did not reveal microfilariae [2],[3] suggest that filaria can exist without microfilaremia. Proportion of cases in endemic regions neither show microfilariae in blood, nor any symptom. [2],[4] Blood eosinophil counts within normal range, as observed in our case, was also reported by Varghese et al . [3] However, Valand et al . [5] demonstrated eosinophilia in their case. These observations suggest that there is no consistent relationship between filarial infection and blood eosinophilia, which in turn reflects the difference in host response to parasite from person to person. Diagnosis of filarial infection by detection of antigen would obviate the problem in low level of microfilaremia, but such tests are available only in reference laboratory and are expensive. [1] High index of suspicion is required to diagnose such unusual presentation of Wuchereria bancrofti . Careful screening of cytological smear can render definitive diagnosis of early, asymptomatic and clinically unsuspected cases of bancroftian filariasis, especially in those cases where microfilariae is absent in peripheral blood. Acknowledgment Authors are very thankful to Dr. MVR Reddy, Professor and Head of the Department Biochemistry and JB Tropical Disease Research Centre, MGIMS Sevagram for conducting the serological test. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09112f2.jpg] [mb09112f1.jpg] |
| |||||||||

{kind=link}
{kind=link}