 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
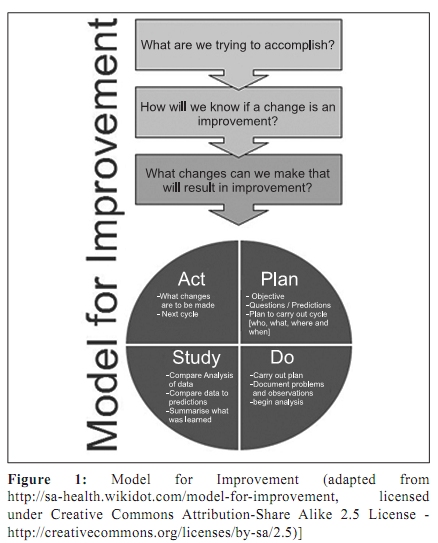
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 11-16 Special Article Infection control with limited resources: Why and how to make it possible? *JB Sarma, GU Ahmed Northumbria Healthcare NHS Foundation Trust (JBS), Rake Lane, NE288NH, England. Department of Biotechnology (GA), Guwahati University, Jalukbari, Guwahati - 781 014, Assam, India Correspondence Address: *Northumbria Healthcare NHS Foundation Trust, Rake Lane, NE288NH, England, jayanta.sarma@nhs.net Date of Submission: 03-Jul-2009 Code Number: mb10004 PMID: 20061756 DOI: 10.4103/0255-0857.58721 Abstract The risk of healthcare-associated infections (HCAIs) in developing countries can exceed 25% compared to developed countries. Lack of awareness and institutional framework to deal with patient safety in general and HCAI in particular perpetuates the culture of acceptance of avoidable risks as inevitable. Most HCAIs are avoidable and can be prevented by relatively simple means. It is no longer acceptable to put patients at risk of avoidable infections. The World Health Organization (WHO)-led World Alliance for Patient Safety launched a worldwide campaign on patient safety focusing on simple means like hand hygiene to combat HCAIs. To drive necessary changes to deliver sustainable improvement in clinical care requires strategic approach and clinical leadership. This article reviews the scale of the problem, the WHO recommended interventions and improvement strategies in institutional setup in developing and transitional countries. Keywords: Cross infection, hand hygiene, improvement methods, infection control, patient care Introduction At any time, over 1.4 million people worldwide suffer from HCAI. About 5-10% of patients admitted to modern hospitals in the developed world acquire one or more infections. [1] In the United States, one out of every 136 hospital patients becomes seriously ill as a result of an infection acquired in hospital; this is equivalent to two million cases and about 80000 deaths a year. In England, more than 100000 cases of HCAIs lead to over 5000 deaths directly attributed to infection each year. HCAIs in England are estimated to cost £1 billion a year. In the United States, the estimate is between US$ 4.5 billion and US$ 5.7 billion per year. In Mexico, the annual cost approaches US$ 1.5 billion. In Mexico, an estimated 450 000 cases of health care-associated infection cause 32 deaths per 100 000 inhabitants each year. [1] The risk of HCAI in developing countries is 2 to 20 times higher than in developed countries; in some countries, the proportion can exceed 25%. [1] A surveillance conducted in 12 ICUs of the seven hospitals of seven Indian cities found 87.5% of all S. aureus HCAIs were caused by meticillin-resistant (MRSA) strains, and 71.4% of Enterobacteriaceae were multi-resistant; the study concluded that HCAI rates, length of stay, mortality and bacterial resistance were high and infection control programmes including surveillance and antibiotic policies are a priority in India. [2] The proportion of HCAI cases potentially preventable under routine working conditions is significant. The 1985 landmark SENIC study [3] showed that with intensive infection control and surveillance programmes, an overall reduction of 32% in HCAI rates could be obtained in a five-year period. A more recent review found a minimum reduction effect of 10% to a maximum of 70%, depending on the setting, study design, baseline infection rates and type of infection. [4] World alliance for patient safety ( www.who.int/patientsafety ) In 2004, WHO launched the World Alliance for Patient Safety in response to a World Health Assembly Resolution (2002) urging the WHO and Member States to pay the closest possible attention to the problem of patient safety. The Global Patient Safety Challenge is a core programme of the World Alliance for Patient Safety aimed at drawing attention to patient safety. The first campaign launched in 2005-06 brings together the WHO Guidelines on Hand Hygiene in Healthcare with ongoing work on blood safety, injection and immunization safety, safer clinical practices, safe water, sanitation and health care waste management. The core message of the campaign is: 'simple measures save lives' which focus on preventing HCAI by simple intervention like hand hygiene. [5] The second challenge, Safe Surgery Saves Lives, commenced in 2007 and was formally launched in 2008. The third challenge, to be launched in 2010, will focus on the unprecedented spread of drug-resistant pathogens and the implications for patient safety. Over 120 WHO Member States have now signed a national pledge to tackle HCAI including India. [6] Is infection control a 'Resource Issue'? Over the last few years, the rate HCAIs has emerged as one of the leading markers of quality of clinical care and patient safety. Infection control underpins 'safe and sound' clinical practice and requires attention to certain details, the responsibility for which lies with every healthcare practitioner. But it is the role of a good management to raise awareness to the problem and make individuals and teams own up responsibility. Lack of awareness is a direct consequence of lack of measurement i.e., unavailability of surveillance data on HCAIs at local level. Although surgical site infections, urinary tract infections, hospital acquired pneumonia including ventilator associated pneumonia and intra-venous device associated infections are of common occurrence, often with serious consequences contributing to mortality and morbidity, clinicians accept these consequences as inevitable part of clinical practice. Lack of institutional framework or programme to deal with such avoidable risks perpetuates the culture of acceptance of HCAIs as inevitable consequence. Another factor is inadequate microbiology laboratory services and lack of clinical microbiology expertise. That the incidence of infections with multi-resistant nosocomial pathogens such as Meticillin Resistant S. aureus or extended spectrum β-lactamase producing enteric gram negative bacteria are high in the hospital require microbiological confirmation to establish. However, it is possible to carry out surveillance of HCAIs even in the absence of microbiological confirmation - a physician or surgeon diagnosis of infection derived from direct observation or from clinical judgment is an acceptable criterion for an HCAI. [7] Healthcare-associated infection: marker of quality of clinical care Infection control and prevention is fundamental to improving care and ensuring safety. A safer clinical care environment and adherence to certain basic principles already address many issues related to infection control. However, it is learnt from the recent experience in the developed countries that it is possible to lower the HCAI rate only when infection control is accepted as a core corporate and individual responsibility by both the management and clinical staff facilitated by an infection control team (ICT) under a formal institutional programme. The ICT is a source of expert knowledge and help but the responsibility must lie with the clinical team. It is also a requirement that the effort to combat HCAIs is whole heartedly backed by the management and made a priority and a core standard to be achieved. [8],[9] In England, safeguarding patients and staff from the risk of avoidable HCAIs has recently been made a statutory responsibility of the hospital management. [10] Driving changes to combat healthcare-associated infection Driving changes and making improvement in a complex organisation such as a hospital is a challenging task, particularly when it comes to a problem like HCAIs where change in attitude and behaviour by the all concerned are critical in dictating success or failure. Innovation and improvement Investment in infrastructure and equipment is necessary, but there is also a need to put in continuous effort to make incremental improvement of the services within the available resources and constraints. Reducing incidence of HCAIs is considered an integral part of patient safety and quality of care. As such, the hospital needs to embark on a planned 'quality improvement programme' that incorporates reducing HCAIs as priority. Improvement methods Any improvement process is driven by a team led by effective leadership, with a commitment of adequate resources and attention by the management. A successful team is multidisciplinary that sets clear aims for their work, establishes baseline measurements, regularly measures and studies the results, and tests various process and systems changes over a variety of conditions to find the ones that lead to improvement in their particular setting [Figure - 1]. [11] The Model for Improvement [12] is a simple yet powerful tool for accelerating improvement. This model has been used very successfully by hundreds of health care organizations in many countries, both developed and developing, to improve many different health care processes and outcomes. The model has two parts:
The web-based learning on the 'How to of Improvement' developed by the Healthcare Improvement Skills Centre ( www.improvementskills.org ) is a very useful and highly recommended resource for the healthcare personals. These modules are intended to advance a provider's ability to recognise, analyse, and improve quality improvement opportunities in their organization. Institute of healthcare improvement ( www.ihi.org ) also offers a comprehensive web-based training on the model for improvement, a tool for making rapid improvement in care. Setting up an infection control programme Infection Control Doctor (ICD) and Infection Control Nurses (ICN) are specialists in infection control. In developed countries the hospital infection control programme is led by a specialist Infection Control Team (ICT). It is essential that the hospital formally sets up an infection control programme and follows the model of improvement to develop the programme. The first step will be to form a multidisciplinary ICT and allow the members time and resources to develop necessary skills and orientation, and a plan. There are sufficient free information resources available [13] to help acquire knowledge and competencies. The team will inevitably mature and continue to acquire new skills and insight as they continue to confront practical problems on the ground. The management must ensure that the team has its and senior doctors' full support. Membership of the infection control team Director: A senior doctor who has a senior management role is ideal for this position. Director is expected to provide the system leadership. This person must possess enough authority to institute a change and overcome barriers that may arise. Infection Control Doctor: ICD is ideally a clinical microbiologist who is the technical expert and knows the subject intimately and understands the processes of care. Lead Infection Control Nurse Specialist: This role is expected to provide day-to-day leadership assuring that tasks are implemented and necessary data being collected. Infection Prevention and Control Nurses (one assigned per project location/ward/department): They are expected to collect surveillance data and provide hands on training and advice to the frontline staff on a daily basis. Antibiotic Specialist: A senior physician/microbiologist with interest and expertise, who is expected to provide leadership to develop hospital antibiotic policy and guidelines for the management of infections. Team Administrator: An individual with necessary IT skills who is able to produce spread sheets and present data in graphical format using simple statistical software package like Excel. An expert (optional) on improvement methods can provide additional technical support by helping the team determine what to measure, assisting in design of simple, effective measurement tools, and providing guidance on collection, interpretation, and display of data. Setting the aims The ICT should initially set a few clear aims, time-specific and measurable, targeting a specific population of patients or locations. Modest aims e.g., the following two could be set to start with:
'There may be infection control without surveillance, but those who practice without measurement will be like crew of an orbiting ship travelling through space without instruments, unable to identify their current bearings, the probability of hazard, their direction or rate of travel'-Richard Wenzel. Establishing rate of HCAIs via surveillance is necessary to determine the scale of the problem and demonstrate that improvement is taking place (reducing rate of HCAI) as a result of the interventions put in place. Establishing measure is the only way to show that changes made are actually leading to an improvement. The surveillance strategy should be selected carefully depending on available resources and the situation; 'targeted outcome surveillance' and 'process surveillance' (or clinical audit) are considered appropriate when resources are limited. [14],[15]
Considering the two examples cited above, the following interventions would be appropriate:
According to the principle of the Plan-Do-Study-Act (PDSA) cycle, the ICT will carry these interventions on a small scale in the specified locations and learn from the results and refine the changes if desired improvement is not achieved. In summary, the strategy can be described as follows:
Once PDSA cycle is successful, the team can implement the interventions on a broader scale extending to more locations. Eventually, the team can spread the changes even more widely as the interventions have now proved robust and effective enough, which may even encourage similar hospitals to emulate the changes to achieve improvement. Need for Specific Urgent Initiatives The first global patient safety challenge "Clean Care is Safer Care" Every hospital should launch the WHO sponsored 'Clean Care is Safer Care' campaign as a matter of urgency. 'Clean Care is Safer Care' addresses an issue of universal relevance to patient safety aimed at reducing HCAIs worldwide. The main plank of the campaign is 'Five Moments for Hand Hygiene' approach. [16] Quite simply, it defines the key moments for hand hygiene, overcoming misleading language and complicated descriptions. It presents a unified vision and promotes a strong sense of ownership. A range of tools and resources have been developed to complement the Five Moments approach including localised country specific tool. [23] Alcohol-based handrubs Five Moments for hand hygiene put a great emphasis on alcohol-based handrub. Proper use of alcohol-based handrub renders the hands safe in terms of transmission of pathogens, and can be used at the very place where pathogens are transmitted viz., point of care. It is unlikely, although, not impossible, that running water, soap and paper towels will be installed right at the point of care. At the present time, the most efficacious, well-tolerated and well-researched product which can be placed ergonomically and safely at the point of care is an alcohol-based handrub. In countries where access to sinks is limited or non-existent, alcohol-based handrub offers a method of preventing cross-infection which can be implemented immediately while sufficient numbers of clinical hand wash sinks are being installed. [5] It has revolutionised hand hygiene improvement strategies in the modern age, although need clean hands with soap and water at certain times remains (e.g., when hands are visibly dirty or exposure to potential spore-forming organisms is suspected or proven, or after using the lavatory). Making alcohol-based handrub available at affordable cost The WHO recommended handrub formulations meet both US and European norms which can be easily produced locally by hospitals instead of buying expensive commercial formulations. [5] Commercial alcohol-based handrub products tend to be costly in India for large scale consumption. Handrub formulations based on the WHO formula can be manufactured within the hospital in an on-site pharmacy laboratory. Alternatively, a group of hospitals can contract production to local manufacturers which will save money and ensure steady supply. Establishing Clinical Microbiology Laboratory Capacity Building and running a clinical microbiology laboratory services could be challenging. Technical as well as clinical expertise in diagnostic microbiology can be built over a period of time. Without clinical expertise a laboratory will test each and every specimen (influenced perhaps by element of commercial motive) sent rather than guided by a screening and rejection criteria for specimens that address certain questions: Will the results alter patient management? What is the public health importance? What is the relative yield of a Gram-stained smear versus a complete culture? It may not be clinically beneficial testing inappropriate specimens apart from the cost involved. One approach could be to build capacity starting with cohort-based studies to establish the causes and clinical predictors for HCAI and thereby facilitate directed rather than blind empiric therapy. [24] Emphasis should be initially on to perform quality-controlled laboratory testing for a finite period, rather than ongoing routine individual patient-directed diagnostic testing, as part of a cohort-based study acting as a surveillance 'probe' providing useful clinical and public health information, determining the true incidence and prevalence rates of nosocomial pathogens and antimicrobial-drug resistance, and yielding clinical predictors for various HCAIs in defined patient cohorts. These studies provide the opportunity to establish diagnostic capability and build clinical expertise in basic clinical microbiology in the hospital or laboratory. The hospital management must be willing to fund these studies as the eventual benefit will be long lasting and sustainable. Indian Context: Specific Considerations and Role of Microbiologists Experience from the developed countries suggests that HCAI control programme performs best if the frontline clinical staff own the responsibility with the ICT providing expert support acting as facilitator. Microbiologists in Indian hospitals, who are medically qualified, are in pole position to provide leadership to help form an interdisciplinary hospital ICT and develop an effective programme. While continuing to strive towards developing a capable and quality clinical microbiology laboratory service, critically, they have to engage themselves in clinical liaison interpreting laboratory results, guiding antibiotic therapy and providing infection control advice, which could well be unsolicited, to create a niche and develop a role they can play in saving lives. This is challenging given the traditional clout physicians and surgeons enjoy who might see this as an invasion on the part of the microbiologists. Irrespective, taking the initiative when the climate is right and need is the most is the logical choice. As discussed in this paper, a systematic approach starting with establishing the scale of the problem in one's local hospital is critical to persuade and engage the management and clinical colleagues in an improvement process. The Indian microbiologists need to demonstrate leadership in this regard and work hard to curve a role for themselves as experts and facilitators in the process making the management and clinical teams to own up responsibility. Undoubtedly, new competencies are required to meet the requirement of this new role outside the comfort zone of the laboratory which have to be gained through self directed CME and CPD activities. The professional bodies of Indian microbiologists must play its role in making CME and CPD activities available to help acquire new competencies, and in drawing up a model job description for hospital microbiologists encompassing this new 'aspirational' role in addition to work with the Indian Medical Council to update MD Microbiology curriculum so that the new generation of medical microbiologists are up to the challenges. Summary It is not a matter of cost but lack of awareness and recognition of HCAIs as a major risk putting patients' lives at risk which is unacceptable. The scientific, technical and educational resources and examples of successes elsewhere are available to emulate with necessary innovation and variation to meet the local challenge. Increasing public awareness will inevitably lead to enactment of new legal framework requiring hospitals to prevent HCAIs as a matter of legal responsibility in India similar to country like England. With increasing awareness, victims of HCAIs are likely to increasingly resort to existing legal remedies such as consumer protection act. It is high time that the medical profession in India turns its attention to the menace of HCAIs and provides the much needed leadership. Indian microbiologists are in a unique position to take leadership role in this high priority area of patient safety and reducing harms from avoidable HCAIs. Acknowledgement The paper was commissioned by North East Clinical Excellence Foundation ( http://www.necef.in ) References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10004f1.jpg] |
| |||||||||
{kind=link}