 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
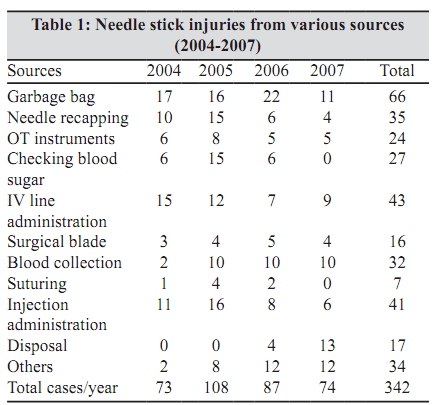
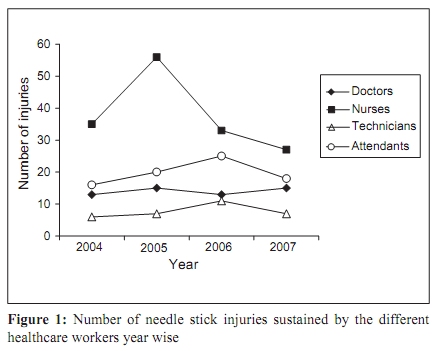
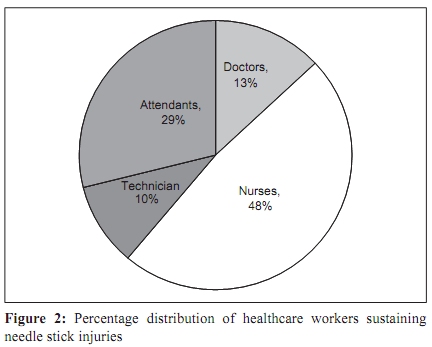
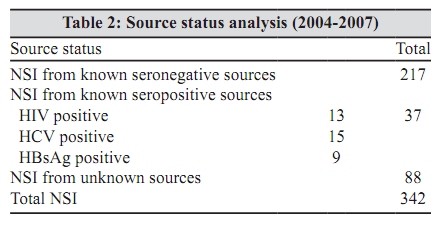
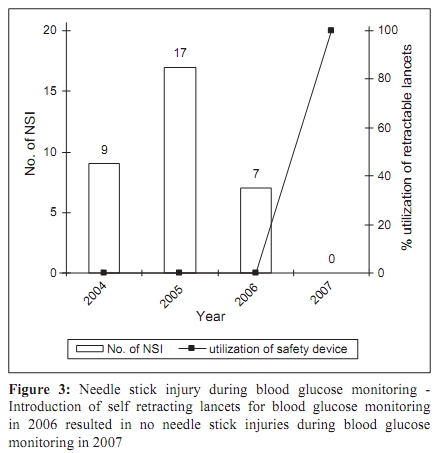
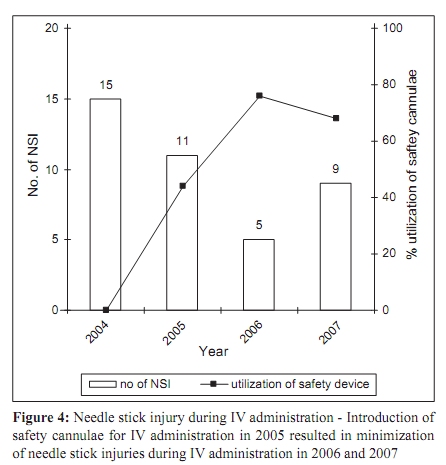
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 17-20 Original Article Interventions to reduce needle stick injuries at a tertiary care centre *A Mehta, C Rodrigues, T Singhal, N Lopes, N D’Souza, K Sathe, FD Dastur Department of Microbiology, P.D. Hinduja National Hospital and Medical Research Centre, Veer Savarkar Marg, Mahim (West), Mumbai - 400 016, India Correspondence Address: *Department of Microbiology, P.D. Hinduja National Hospital and Medical Research Centre, Veer Savarkar Marg, Mahim (West), Mumbai - 400 016, India, dr.ajita.mehta@gmail.com Date of Submission: 19-Aug-2008 Code Number: mb10005 PMID: 20061757 DOI: 10.4103/0255-0857.58722 Abstract Background: Occupational exposure to blood/body fluids is associated with risk of infection with blood borne pathogens like human immunodeficiency virus (HIV), hepatitis B virus (HBV) and hepatitis C virus (HCV). Keywords: Blood borne pathogens, hepatitis B virus, human immunodeficiency virus, occupational exposure, post exposure prophylaxis Introduction Percutaneous injury with an infected sharp device can lead to exposure of the HCW to various blood borne pathogens like hepatitis B virus (HBV), hepatitis C virus (HCV) and human immunodeficiency virus (HIV). The first report of HIV transmitted to a HCW as a result of a NSI was published in 1984. [1] The World Health Report 2002 estimates that 2.5% of HIV, 40% of HBV and HCV cases among HCWs worldwide are the result of occupational exposures. [2] The absence of appropriate post exposure prophylaxis (PEP) in such exposures is associated with enhanced risk of infection with these pathogens. The emotional impact of a needle stick injury can result in considerable psychological trauma for the HCW. [3] Data from developing countries show that adherence to 'universal precautions' and documentation of exposures are suboptimal and also that awareness about PEP among HCWs is poor. [4],[5] There are very few studies in India documenting the frequency, PEP protocols followed and consequences of needle stick injuries. [6],[7],[8],[9],[10] Studies show that many of the occupational exposures that occur in hospital go unreported, and thus the number of infected individuals may be much higher that the Figures actually reported. [8],[11],[12] At our centre, since the past several years, we have a defined policy to prevent, report and manage occupational exposure to blood borne pathogens. Results of such as a surveillance study have been reported in an earlier communication. [13] We now report further surveillance data, along with interventions introduced to reduce needle stick injury, and collate the results of a continuing study over the past four years. Materials and Methods This study was carried out at a 351 bedded tertiary care hospital in Mumbai, India. All occupational exposure to blood and body fluids are managed as per the hospital guidelines. Following injury, HCWs were instructed to thoroughly wash the site with water and soap or an antiseptic solution, encourage bleeding of the site, avoid squeezing the site and immediately report to the hospital casualty/emergency room. The HCWs gave the casualty officer a detailed account of the exposure along with their hepatitis B immunization status. The type of injury and degree of exposure is also recorded along with the device of exposure on a reporting form. If the exposure occurred from a known source, the source's blood was collected for HIV, HBV and HCV testing. Simultaneously; the HCWs blood was also collected. If the source blood tested negative, the HCWs blood is not tested further. If the source blood is positive for HBV/HCV/HIV, the HCWs blood is also tested for baseline serostatus. Appropriate PEP, as recommended by the Centres for Disease Control (CDC) [13] and as reported earlier in our previous communication, [14] is administered to the affected HCW. Infection control nurse (ICN) and chairperson, infection control committee (ICC), are informed about the incident. All follow-up is carried out by the ICN for the affected HCWs. When the source of exposure is unknown and the HCW has not received immunization, HBV vaccination is initiated. HIV prophylaxis is not initiated unless there is reason to believe the exposure was associated with a sharp object infected with HIV. Since 1998, we have been conducting a monthly compulsory induction programme for all HCWs on employment. An annual "Infection Prevention week" is also conducted by the infection control committee, which benefits all HCWs, and significantly aids in creating an all round awareness about the different aspects of infection control. The programme is conducted with different sessions for the doctors, nurses, technicians and housekeeping staff with many sessions taken by each of those HCWs to ensure that relevant topics are covered in various aspects to benefit that specific group. Our hospital has special colour coded disposal bags for different types of waste and puncture proof containers meant for the disposal of sharps. Segregation of waste at source, especially sharps, is very important in minimizing NSI from garbage bags for the housekeeping attendants. HCWs are educated on the need to safely comply with universal precautions and take the utmost care, especially while disposing sharps. Creating awareness about good waste management ensures the proper disposal of sharps that helps prevent needle stick injuries from sources like garbage bags, injuries sustained while recapping needles and during injection administration. Various interventions have been made over the years by the ICC to help minimize the risk of sharp injury. After it was observed that many nurses suffered sharp injuries while pricking a patient for blood glucose monitoring, the ICC decided to replace the needles used with self-retracting lancets, in 2006, to try and minimize risk of injury during glucose monitoring. Similarly, the ICC introduced safety cannulae, in 2005, to see if this would reduce injuries during IV administration. Results Three hundred and forty two cases of NSIs were reported at our hospital in the past four years (2004-2007). The largest number of sharp injuries were sustained through garbage bags (N = 66) followed by those during IV line administration (N = 43), injection administration (N = 41), needle recapping (N = 35), blood collection (N = 32) and blood sugar monitoring (N = 27). Needle stick injuries were also sustained from OT instruments (N = 24), during disposal of needles (N = 17), using surgical blades (N = 16), suturing (N = 7) and from miscellaneous sources (N = 34) [Table - 1]. Most needle stick injuries involved the hospital nurses (44%) and attendants (23%). Other HCWs who sustained sharp injuries were doctors (16%) and technicians (9%) [Figure - 1] and [Figure - 2]. Of the 342 sharp injuries, 254 were from known sources and 88 from unknown sources. Of the known sources, 37 were seropositive [HIV (13), HCV (15) and HBsAg (9)] [Table - 2]. None of the HCWs exposed to a positive source was positive at baseline for HBV/HCV/HIV. Appropriate PEP, as defined earlier, was initiated in all positive exposures. Of the nine HCWs exposed to HBsAg positive sources, eight had completed their immunization series and had a good antiHBs titre; hence they were given no PEP. However, one HCW was a new employee having just taken the first HBV immunization dose and was antiHBs negative. Consequently, he was administered the hepatitis B immunoglobulin (HBIG) and his vaccination was continued as per schedule. Of the 13 HCWs exposed to HIV positive sources, nine were given anti retroviral therapy (ART). The basic ART regime (consisting of the nucleoside reverse transcriptase inhibitors, Zidovudine and Lamivudine) was given to seven HCWs and the expanded regime (consisting of Zidovudine and Lamivudine along with a protease inhibitor like Indinavir) was administered to two HCWs by the physician as per the exposure code. Three HCWs who sustained injuries from HIV positive sources were lost to follow-up. One HCW developed rashes while taking the basic ART regime. The 15 HCWs who sustained injuries from HCV positive sources were followed up by the Gastroenterology team with liver function tests. Follow-up is complete till date for all HCWs who sustained NSIs. There has not been a single case of seroconversion till date. Discussion In this first surveillance study of its kind from an Indian institution, we report a universally successful outcome of occupational exposure to blood borne pathogens. Prevention and management of occupational exposures has been a thrust area of the hospital infection control committee since the last several years. Continuing education and training for HCWs has been very successfully carried out at our institute for many years. There has been a decline in sharps injuries from garbage bags, needle recapping and during injection administration, over the years due to constant awareness programs conducted at our hospital on infection control. Regular education is also very important to discourage practices like needle recapping and encourage responsible storage, use and disposal of sharps. Since the introduction of self retracting lancets for blood glucose monitoring, there has not been a single needle stick injury during this activity till date [Figure - 3]. Introduction of safety cannulae has reduced the number of sharp injuries sustained during intravenous IV cannulation. In 2004 there were 15 needle stick injuries during IV cannulation. By 2005 there was only 44% utilization of the safety cannula and sharp injuries had gone down till 12. In 2006 the utilization had gone up till 76% and the number of injuries had gone down to seven in 2006. In 2007 the safety cannulae utilization was 65% and there were nine injuries [Figure - 4]. Since 2005 the total numbers of nurses sustaining NSI have also reduced appreciably due to constant educational programs and the introduction of safer devices in our hospital [Figure - 1]. The ICC at our hospital constantly strives to introduce interventions in the hospital so as to safeguard the health of its staff. Only constant surveillance can ascertain exactly what interventions are wise to make and wither they are resultant in a positive change. Even after the introduction of safety devices, it must be kept in mind that needle stick injuries can take place if these devices are not used and disposed of properly. Hence the staff concerned need to be well trained to use such devices before these can be introduced into habitual usage in the hospital. Training programmes need to be organized constantly, especially in countries like India where the staff turnover, especially that of nurses is very high and these new HCWs might be completely alien to using new and safer devices. At our hospital we stress very strongly on an induction programme for all HCWs on employment which aids significantly in getting them accustomed to the working principles. The HCWs anti-HBS status is evaluated on employment and their HBV vaccination series is started if they haven't been vaccinated in the past. This ensures that all HCWs are protected against HBV. Other programmes like the "Infection prevention week," conducted annually, also helps all the HCWs at our hospital maintain an all round awareness on the various aspects like; proper waste and sharps disposal, universal precautions, occupational exposure to blood/body fluids, airborne infections like tuberculosis which could afflict HCWs and other vital issues. Conclusions This surveillance study accentuates the fact that occupational exposures can be reduced and it is vital for all hospitals to have a proper occupational health policy in place. Universal HBV vaccination of all HCWs, continuous education and training, introduction of safety devices, appropriate waste and sharp disposal, ensuring reporting of all exposures, institution of appropriate PEP, psychological support and counselling of affected HCWs and stringent follow-up are all needed to reduce the burden of occupationally acquired infections in HCWs. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10005t2.jpg] [mb10005f2.jpg] [mb10005t1.jpg] [mb10005f1.jpg] [mb10005f4.jpg] [mb10005f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}