 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 21-25 Original Article Effectiveness of anti-tuberculosis treatment among patients receiving highly active antiretroviral therapy at Vihiga District Hospital in 2007 SO Kwange, *NLM Budambula Medical Microbiology Sub-Department (SOK), Department of Botany (NLMB), Jomo Kenyatta University of Agriculture and Technology, P.O Box 62000, Postal code 00200, Nairobi, Kenya Correspondence Address: *Medical Microbiology Sub-Department (SOK), Department of Botany (NLMB), Jomo Kenyatta University of Agriculture and Technology, P.O Box 62000, Postal code 00200, Nairobi, Kenya, nbudambula@yahoo.com Date of Submission: 10-Mar-2009 Code Number: mb10006 PMID: 20061758 DOI: 10.4103/0255-0857.58723 Abstract Purpose: In Kenya there is need for proper co-ordination of antiretroviral therapy (ART) and tuberculosis (TB) treatment as most (60%) of the TB patients are also human immunodeficiency virus (HIV) positive. This study aims to determine the difference in response to TB treatment among HIV-negative TB patients and HIV-positive TB patients receiving delayed highly active antiretroviral therapy (HAART) at Vihiga District Hospital. Keywords: Antiretroviral therapy, human immunodeficiency virus, tuberculosis Introduction Effective therapy is available for both tuberculosis and human immunodeficiency virus (HIV), but there are major challenges in the concurrent treatment of HIV and TB co-infection. HIV-positive patients with tuberculosis (TB) are all potentially eligible for ART, because they are in either World Health Organization (WHO) Clinical Stage 3 (pulmonary tuberculosis [PTB]) or Stage 4 (extra-pulmonary tuberculosis [EPTB]). HIV-positive TB patients benefit from ART, which leads to a reduction in HIV-related mortality and HIV-related recurrence of TB disease. [1] HIV infection is a key factor responsible for increasing the rates of TB in developing countries in sub-Saharan Africa. At the time of TB diagnosis, most patients with co-infection have advanced HIV disease characterized by low CD4 cell counts and high viral loads. [2],[3] The development of active TB, on the other hand, is associated with increases in HIV viral load locally and systemically. [4],[5] The HIV epidemic is fueling the TB epidemic mainly in Sub-Saharan Africa, Kenya in particular, where the TB Case Notification Rate (CNR) has steadily increased from 54 per 100,000 in 1991 to 329 per 100,000 in 2006, mainly due to HIV. In 1994, a national survey to determine the prevalence of HIV among TB patients in Kenya had found that 40% of TB patients were HIV seropositive. Recent estimates indicate that 60% of TB patients in Kenya are co-infected with HIV. [6] The earlier guidelines of the American Thoracic Society, Centers for Disease Control and Prevention (CDC) and Infectious Diseases Society of America TB treatment suggested that delaying the initiation of antiretroviral therapy until four to eight weeks after starting anti-tuberculosis therapy would allow for better evaluation of drug side effects, and reduce the severity of paradoxical reactions and adherence difficulties for the patient. This recommendation was based largely on the high rates of treatment discontinuation due to adverse effects, and concerns about adherence when multiple medications were started at the same time. [7] However, there is no recommendation on when to start HAART in TB-HIV patients in the latest guidelines, because it is not well known. [8] Vihiga District in Western Kenya has recorded a sharp increase in TB cases over the last decade and some of these patients are now on ART. However, information on the response of these patients to TB treatment while receiving HAART is scanty. The aim of this study was to determine the difference in response to TB treatment among HIV-negative TB patients and HIV-positive TB patients receiving delayed HAART at the Vihiga District Hospital. Materials and Methods Design This was an analytical study designed as a prospective cohort of smear positive pulmonary tuberculosis (PTB) patients undergoing chemotherapy at the Vihiga District Hospital in Western Kenya. Setting This study was carried out at the Vihiga District Hospital, Kenya, in the Skin and Chest Clinic and in collaboration with Voluntary Counselling and Testing (VCT) and Laboratory Departments of the Hospital. Subject recruitment and treatment Patients with pulmonary tuberculosis (PTB) were diagnosed and enrolled for the study from 15 January, 2007 to 28 February, 2007. The inclusion criterion was set as follows: Only smear positive TB patients who were registered and were getting their treatment at the Vihiga District Hospital and only new PTB patients were considered, that is, they must not have had TB or TB or ART treatment before and they had to be PTB patients of age 15 years and above. In addition only patients who consented were enrolled in the study. The TB patients were also offered HIV testing and counselling through the process of Diagnostic Testing and Counselling (DTC), and then categorized into category A (PTB with HIV) and category B (PTB without HIV co-infection). The sample size was calculated using the formula by Harper (1980) as follows:
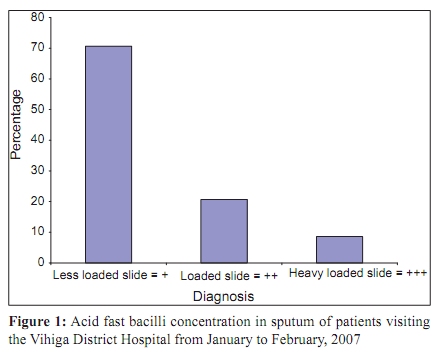
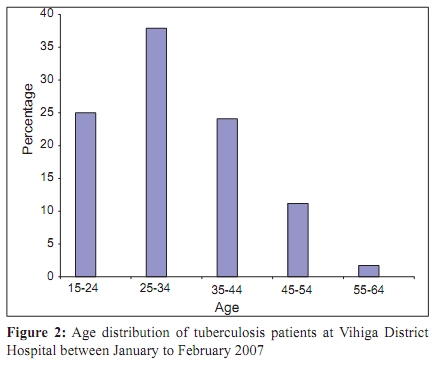
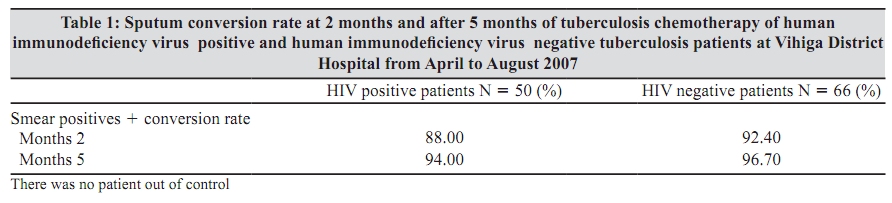
The actual number of cases of the subjects that were enrolled for the study was as follows: HIV positive TB patients (n = 50) and HIV negative TB patients (n = 66). The patients were then put on the same TB chemotherapy of short course (2RHZE + 6EH) comprising of the following drugs as recommended by National Leprosy and Tuberculosis Program (NLTP): Two months of Rifampicin-R, Isoniazid-H, Pyrazinamide-Z and plain Ethambutal-E, and then six months of Ethambutal and Isoniazid. The dosage was calculated per kilogram of body weight of the patient and the medication was taken daily at the same time by the patient, under the supervision of a healthcare worker or any other responsible family member (DOTS). The HIV positive TB patients were referred to the ART centre. At the ART centre HAART was delayed for four to eight weeks after the initiation of TB treatment. The recommended national first line regimens for TB patients starting antiretroviral therapy treatment while on rifampicin was d4t (stavudine) +3TC (lamuvudine) + EFV (efavirenz) were adhered to. For patients who were no longer on rifampicin the standard regimen of d4t (stavudine) + (lamivudine) +NVP (nevirapine) was administered as per the revised NLTP Guidelines. [6] The two categories of patients were monitored for bacteriological response at two months and after five months of TB chemotherapy in which the patients' follow up sputum smears were examined microscopically for Acid Fast Bacilli (AFB). The main outcome measure in this study was the sputum conversion rate from positive sputum to negative sputum during the intensive phase of chemotherapy and the results were recorded on the prescribed form. Specimen (Sputum) collection and data collection At diagnosis three sputum specimens were collected from all patients as follows: One spot specimen when the patient first attended the clinic, one early morning specimen and one spot specimen when the early morning was submitted to the laboratory, summarized as Spot + Morning + Spot. Direct smears from each sputum specimen were prepared and stained using the Ziehl-Neelsen procedure. A suspect was diagnosed as a smear-positive TB patient when at least one of the three smears was positive by the Ziehl-Neelsen procedure. Reporting of results was done using the WHO guidelines on TB reporting. Data analysis Each category of patient's age, gender, diagnosis (AFB results), HIV status, AFB results at two months and AFB results after five months were coded and assigned numbers for ease of data entry and processing. SPSS for windows, version 12.0 computer software was then used for entering, processing and data analysis. Both qualitative and quantitative approaches were used to compare the variables. The data was subjected to one-way ANOVA, to determine the differences between the outcomes of the combined groups, with HIV-status as grouped data. The statistical significance level was 0.05. Scientific ethics Permission to carry out this research, accumulate data and publish the findings was granted in writing by the Office of the Medical Superintendent. The research proposal was presented to the Departmental Panel at Jomo Kenyatta University of Agriculture and approved. Among the issues considered by this Panel were safety and ethics. Health workers at the hospital talked to the patients and obtained verbal informed consent from the patients in Kiswahili, which is the national language in Kenya. Where necessary the consent was obtained in Kiluhya the local language. The health workers also collected the sputum. No names were published anywhere during the study so as to conceal the identities of the patients. Results A total of 116 patients suffering from pulmonary tuberculosis were identified at the Vihiga District Hospital between January and February, 2007. Only the smear positive patients getting their treatment at the hospital were enrolled for the study. The TB patients were diagnosed on the strength of the sputum; less loaded slides gave the highest percentage at 71% (82) as shown in [Figure - 1]. Pulmonary tuberculosis (PTB) burden was noted to be high in patients between 15 and 44 years of age, with the highest hit age group being 25 to 34 years, accounting for 38% of the total cases diagnosed [Figure - 2]. More males were infected giving a higher percentage of 61% (71) than females who gave the lower percentage of 39% (45). Hence male to female ratio of patients with PTB was 1.6:1. The sputum conversion rate at two months and after five months for HIV-positive patients on the anti-TB drugs was 88% (44 of 50) and 94% (47 of 50), respectively. It was observed that n = 2 of the heavily loaded slide of (+++) only reduced to loaded slide (++) while n = 3 reduced to a less loaded slide (+). Despite slow evolution all the slides turned negative after five months. The sputum conversion rate at two months and five months of the HIV-negative patients, 57% (n = 66), on the anti-TB treatment was 92% (61 of 66) and 97% (64 of 66), respectively [Table - 1]. Test of difference in bacteriological response One way analysis of variance (ANOVA) showed that there was no significant difference in the bacteriological outcome responses to TB chemotherapy between the combined groups of HIV-negative TB patients and HIV-positive TB-patients receiving HAART. The probability of the F-ratio at two months and at five months was 0.061 and 0.591, respectively. These were greater than the 0.05 critical value, hence were not statistically significant. Discussion This study recorded a high sputum conversion rate for HIV-positive TB patients on HAART after two months and five months of TB chemotherapy of 88 and 94%, respectively. This rate was comparable to the high sputum conversion rate for HIV-negative TB patients at two months and after five months of 92 and 97%, respectively. Although comparing of sputum smear conversion rates between HIV-seropositive and HIV-seronegative individuals is a well-researched area and its significance is not highlighted in the HAART era, it is an important indicator towards the process, achieving good control of TB and HIV, as part of the collaborative activities of the two diseases. This was well above the minimum WHO recommendation of 85% for good control. [6] High sputum conversion rate that was observed in this study corresponded with treatment adherence, as most of the patients strictly took their medicine as prescribed coupled with the current implemented Direct Observation Therapy (DOT). Smear conversion has been shown to be a critical determinant for successful TB treatment. [9],[10] Smear conversion results may be used for management of patients and for monitoring programme performance. [11] Kenya is yet to achieve the internationally agreed 70/85 TB control targets. The WHO estimates that the Case Detection Rate (CDR) for 2004 was around 47%, while the treatment success rate has been steady at 80% since the adoption of the Directly Observed Therapy Short Course (DOTS). [6] There was no significant difference in the bacteriological outcome responses to TB chemotherapy between the TB patients regardless of their HIV status, since HAART was delayed for up to eight weeks in most (74%) of the HIV-positive TB patients. This minimized the complications of concomitant HAART during TB treatment, as well as promoted adherence during the first two months, which was a critical determinant for the cure of TB. The small difference in the outcome responses observed in the case of difference in slide concentration as a factor where a heavily loaded slide, specifically for the HIV-positive TB patients, signified a well-established infection deep in the lungs characterized with multiplication in the number of bacilli. This advanced kind of infection was difficult to treat and could blunt the protective effect of HAART, but required a longer period. In this study 10% of 50 HIV-seropositive patients with heavy loaded slides (+++) either reduced to less loaded slide (+) or reduced to less than 10 bacilli per slide in a hundred fields viewed microscopically. This was contrary to the rest of the slides, most of which turned negative within the same period. The current provision of anti-retroviral in Kenya's health care system highly recommends that tuberculosis patients with HIV should be offered ART or referred to ART centres at the earliest opportunity. A majority of HIV infected TB patients will initiate ART after the intensive phase of TB treatment and this may be the optimal time for these patients to be referred to ART centres. However, very sick patients may need to initiate ART earlier. [6] The use of HAART in TB-endemic areas has been associated with more than 80% reduction in the incidence of HIV-associated TB; the protective effect of HAART is the greatest in symptomatic patients and those with advanced HIV/AIDS disease. [12] Other studies have reported that the use of concurrent HAART in co-infected patients during TB treatment is associated with reduced mortality. [13],[14],[15],[16] More males were infected than females, possibly because of low sputum positivity among women with TB. Some women could not produce the required quantity of sputum leading to false negative tests, which was more common in women than men. However, data from this study is consistent with other studies that suggest that TB is more a disease of men than of women. [17] This highlights the need for a robust gender analysis to understand the reasons for the differences and to identify the effective points of intervention. Higher rates in men are consistent across different sources of data, including case detection and notification and prevalence surveys, although most have their limitations. There are variations across geographical regions and age groups. Biological functions provide some explanation for the differences; however, there is also an interactive effect with risk and exposure including lifestyle, such as smoking, occupation, indoor air pollutants associated with cooking and from industrial exposure. [18],[19] Overall, results from this study indicate that there is no significant difference in bacteriological outcome responses to TB chemotherapy between the combined groups of patients, regardless of their HIV status. Moreover, the high sputum conversion rate of 92.4% for HIV-positive TB patients and of 94.7% for HIV-negative TB patients after five months of TB chemotherapy indicates good control of TB as recommended by the WHO. Thus, the standard KNTLP regimens [6] are effective in achieving a good cure rate for TB, regardless of ones HIV status. This supports the policy of providing free access to HAART, which may contribute to a reduction in the incidences of TB in populations with a low socioeconomic level and high prevalence of co-infection with HIV and Mycobacterium tuberculosis. Acknowledgement This investigation received financial support from the Jomo Kenyatta University of Agriculture and Technology (JKUAT). References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10006t1.jpg] [mb10006f2.jpg] [mb10006f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}