 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
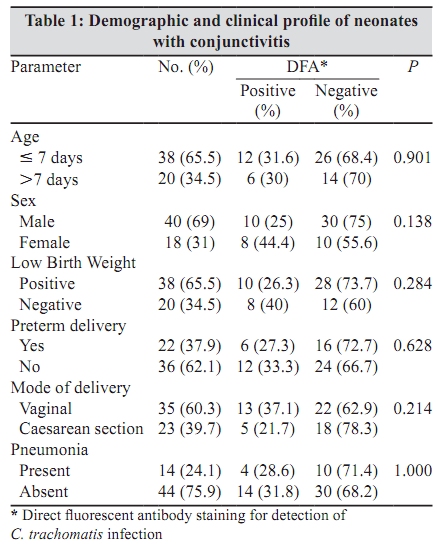
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 45-47 Brief Communication Chlamydia trachomatis causing neonatal conjunctivitis in a tertiary care center S Kakar, *P Bhalla, A Maria, M Rana, R Chawla, NB Mathur Department of Microbiology (SK), Deen Dayal Upadhyaya Hospital, New Delhi -110 064, India. Departments of Microbiology (PB, MR) and Paediatrics (AM, NBM), Maulana Azad Medical College, New Delhi - 110 002, India. Centre for AIDS and Related Diseases (RC), National Institute of Communicable Diseases, New Delhi - 110 002, India Correspondence Address: *Department of Microbiology, Maulana Azad Medical College, New Delhi- 110 002, India, rupenjadhav@yahoo.com Date of Submission: 20-Jan-2009 Code Number: mb10011 PMID: 20061763 DOI: 10.4103/0255-0857.58728 Abstract Chlamydia trachomatis is considered a major aetiological agent of conjunctivitis in newborns. The objective of the present study was to determine the aetiology of neonatal conjunctivitis and clinico-epidemiological correlates of chlamydial ophthalmia neonatorum. Fifty-eight newborns with signs and symptoms of conjunctivitis were studied. Conjunctival specimens were subjected to Gram staining, routine bacteriological culture, culture for Neisseria gonorrhoeae and direct fluorescent antibody (DFA) staining for diagnosis of C. trachomatis infection. C. trachomatis was detected in 18 (31%) neonates. Findings suggest that since C. trachomatis is the most common cause of neonatal conjunctivitis, routine screening and treatment of genital C. trachomatis infection in pregnant women and early diagnosis and treatment of neonatal Chlamydial conjunctivitis may be considered for its prevention and control. Keywords: Chlamydia trachomatis, neonatal conjunctivitis, ophthalmia neonatorum Introduction Purulent conjunctivitis is the most common ocular disease in neonates. [1] There has been a dramatic decrease in the incidence of gonococcal conjunctivitis since the introduction of Crede's silver nitrate prophylaxis. C. trachomatis, which is not affected by Crede's silver nitrate prophylaxis, has become a major cause of neonatal conjunctivitis. [1] It has been estimated that 2-24% of pregnant women have chlamydial cervicitis and that 18-50% of infants born to these mothers develop conjunctivitis while 15-20% of infants develop nasopharyngeal infection and 3-18% develop pneumonia due to C. trachomatis. [2] In a study carried out previously in the same institute, 10% of pregnant women were diagnosed with cervicitis due to C. trachomatis. [3] Various other bacteria commonly isolated form neonates with conjunctivitis include Staphylococcus, Streptococcus and Haemophilus species. [1],[4] Determination of the aetiology of neonatal conjunctivitis would prove invaluable in the initial management and also in prevention of complications. However, even in a developed country like Netherlands, prenatal chlamydial screening and treatment of pregnant women is not a routine practice. [5] The objective of the present study was to determine the aetiology of neonatal conjunctivitis and clinico-epidemiological correlates of chlamydial ophthalmia neonatorum. Materials and Methods Fifty-eight consecutive newborn infants with eye discharge, admitted in the referral neonatal unit of our hospital, were studied after obtaining informed consent from parents. A case of ophthalmia neonatorum was defined as the presence, in an infant less than 30 days old, of clinically apparent ocular discharge (from one or both eyes). Conjunctival specimens were collected using two sterile cotton tipped swabs and a special swab for DFA, rubbed across the mucosa of each eye lid, avoiding contact with the eye lash. The first swab was transported to the laboratory at room temperature and used for aerobic and facultative anaerobic bacterial culture on five per cent sheep blood agar, chocolate agar and thioglycollate broth. The inoculated plates and tubes were incubated at 378C for a minimum of 72 hours before being considered as negative. For isolation of N. gonorrhoea the second swab was placed in Difco™ Amies transport medium (BD Diagnostics, Sparks, MD, USA) and transported to the laboratory for inoculation of Modified Thayer Martin (MTM) medium. The MTM plates were incubated at 358C in three to seven per cent carbon dioxide for 72 hours before being considered negative. The bacterial isolates were identified using standard procedures. The third swab, a special swab provided with the DFA kit, was used to prepare two smears, one for Gram staining and the second for detection of C. trachomatis by direct fluorescent antibody (DFA) staining by using a commercially available kit (Syva MicroTrak; C. trachomatis Direct Specimen test, Behring Diagnostics Inc., Cupertino, CA, USA), which has a reported sensitivity and specificity of 87-100% and 94-97% respectively as compared to culture. [1],[6] The smear for DFA was made by firmly rolling the swab onto a special teflon-coated glass slide covering but remaining within the perimeter of the well. The air-dried smear was fixed with 0.5 ml of methanol at the bedside and then transported to the laboratory. The fixed smear was stored at two to eight degree celsius and processed within seven days. The smear was stained with 30 ΅l of fluorescein-conjugated monoclonal C. trachomatis specific antibody. The slide was incubated for 15 minutes at room temperature in a moist chamber and washed gently with distilled water for 10 seconds. The well was overlaid with one drop of mounting fluid and covered with a cover slip. Positive and negative control slides, procured commercially (Behring Diagnostics Inc., Cupertino, CA, USA), were stained simultaneously. Presence of more than or 10 elementary bodies (EB's) showing characteristic apple green fluorescence was considered as positive. Data was statistically analysed for correlation of chlamydial ophthalmia neonatorum with various demographic and clinical parameters using Chi-square test and Fisher's exact test, as applicable. Results The demographic and clinical profile of neonates with conjunctivitis is given in [Table - 1]. Forty (69%) neonates were males; 22 (37.9%) were preterm; 35 (60.3%) were born through vaginal delivery; 38 (65.5%) had low birth weight; 44 (75.9%) had conjunctivitis alone, while 14 (24.1%) had conjunctivitis with pneumonia; and 38 (65.5%) had onset of conjunctivitis within seven days of birth. Examination of Gram stained smears revealed pus cells in 22 (37.9%) cases. C. trachomatis was detected in 18 (31%) cases, Klebsiella pneumonia in 10 (17.2%), Staphylococcus aureus and Staphylococcus in 4 (6.9%) cases each. Culture for N. gonorrhoeae was negative in all cases. No statistically significant correlation was found between presence of pus cells and detection of C. trachomatis or any other bacterial agent. Ten to twenty EB's were seen in 10 of the C. trachomatis positive smears, 20-30 EB's in four, while more than 100 EB's were seen in four cases. C. trachomatis infection was detected in a higher proportion of females (44.4%) as compared to males (25%). Four neonates with chlamydial conjunctivitis also had pneumonia. Twelve cases of neonatal chlamydial conjunctivitis were less than or seven days old and 10 had a low birth weight. No statistically significant association was found between conjunctival C. trachomatis infection and various demographic and clinical parameters. Discussion C. trachomatis infection of the newborn is acquired from infected birth canal of the mother. Therefore, C. trachomatis infection in the infants is an indirect indicator of genital tract infection in their mothers. Studies have shown that 18-50% infants born to culture positive mothers develop conjunctivitis. [2] As C. trachomatis is now considered the most common cause of sexually transmitted infections in the world, a high prevalence of neonatal C. trachomatis infection is expected. In our study, C. trachomatis antigen could be detected in 31% of neonates presenting with signs and symptoms of conjunctivitis. Other studies have reported a wide range of prevalence of neonatal conjunctival chlamydial infection ranging from 14% to 46%. [1],[4],[7] This could be due to the variation in the prevalence of genital C. trachomatis infection in the local population and because of different laboratory methods used for diagnosis of C. trachomatis infection. Using Polymerase Chain Reaction, C. trachomatis was detected in 27 (64%) of 42 retrospectively studied infants. [5] In our study, no statistically significant association could be demonstrated between neonatal conjunctivitis due to C. trachomatis and various demographic and clinical parameters like gender, age of onset, low birth weight, premature delivery and route of delivery. Similar to our study, another study conducted at New Delhi in the year 2002 also did not find significant association between vaginal delivery and neonatal chlamydial conjunctivitis. [7] Contrary to the findings of our study, in a study conducted in Kenya, significant association was demonstrated between chlamydial ophthalmia neonatorum and low birth weight. [8] In the present study, bacteria other than C. trachomatis could be isolated from 18 (31%) neonates. However, Mohile et al., could isolate bacteria (other than C. trachomatis) from 50% cases of neonatal conjunctivitis. [7] The most common bacterial species cultured from cases of neonatal conjunctivitis was Klebsiella pneumoniae (17.2%). However, other studies have shown a higher frequency of isolation of Staphylococcus, Streptococcus and Haemophilus species from cases of neonatal conjunctivitis. [1],[4],[7] In a study conducted at Hong Kong, C. trachomatis was reported to be the second most common (n = 19, 21%) cause of acute neonatal conjunctivitis after Staphylococcus aureus (n = 32, 36%) [9] . The exact role of K. pneumoniae in the causation of neonatal conjunctivitis should be further investigated in India. It has been suggested that prevention and control of neonatal chlamydial conjunctivitis could be achieved by routine screening and treatment of genital C. trachomatis infection in pregnant women and early diagnosis and treatment of neonatal chlamydial conjunctivitis with oral erythromycin since specific ocular prophylaxis has unknown efficacy. [10] Since C. trachomatis was found to be the most common cause of neonatal conjunctivitis, further studies should be conducted to assess the efficacy of the above mentioned approaches. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10011t1.jpg] |
| |||||||||

{kind=link}