 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
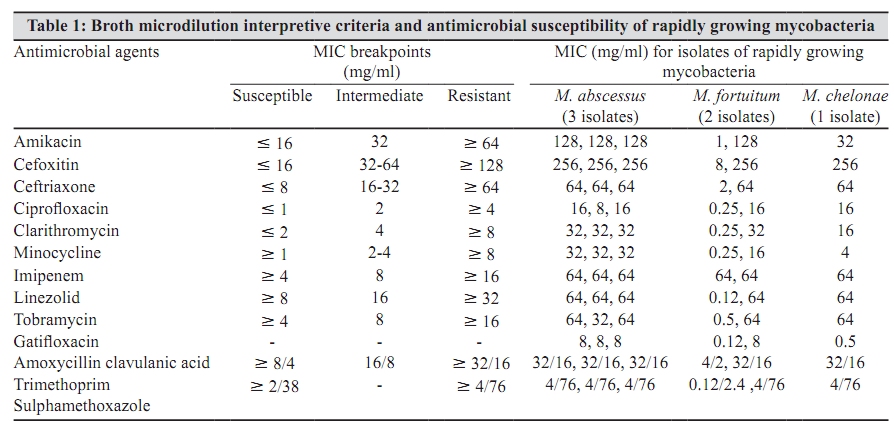
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 48-50 Brief Communication Antimicrobial susceptibility testing of rapidly growing mycobacteria by microdilution - Experience of a tertiary care centre *R Set, S Rokade, S Agrawal, J Shastri Department of Microbiology, T.N. Medical College, Mumbai - 400 008, India Correspondence Address: *Department of Microbiology, T.N. Medical College, Mumbai - 400 008, India, riinaset2001@yahoo.co.in Date of Submission: 17-Nov-2008 Code Number: mb10012 PMID: 20061764 DOI: 10.4103/0255-0857.58729 Abstract Purpose: The objective of the study was to perform antimicrobial susceptibility testing of rapidly growing mycobacteria (RGM) isolated from various clinically suspected cases of extrapulmonary tuberculosis, from January 2007 to April 2008, at a tertiary care centre in Mumbai. Keywords: Antimicrobial susceptibility, broth microdilution, rapidly growing mycobacteria Introduction A wide variety of infections have been associated with rapidly growing mycobacteria, involving the lungs, skin, bones, central nervous system (CNS), prosthetic heart valves, and also in disseminated infections. [1] It is important to distinguish rapidly growing mycobacteria from others quickly, as conventional antituberculous drugs are ineffective for the treatment of infections caused by them. In order to optimize susceptibility testing and facilitate the interpretation of susceptibility results, the Clinical and Laboratory Standards Institute (CLSI) recommends that isolates be identified, at least to differentiate between M. chelonae, M. fortuitum, and M. abscessus. [2] Although there are many reports from India on nontuberculous mycobacteria, the exact burden of disease by rapid growers still remains unclear. We have reviewed the isolation and antimicrobial susceptibility pattern of rapidly growing mycobacteria (RGM) from various clinically suspected cases of extrapulmonary tuberculosis, from January 2007 to April 2008, in the Department of Microbiology at a tertiary care centre in Mumbai. Through this study we wish to emphasize the need to isolate and perform antimicrobial susceptibility tests for RGM from various clinical specimens. Materials and Methods This study included the isolation of RGM from all clinical specimens including lymph node aspirates, pus, tissue, urine, and sterile body fluids of suspected cases of extrapulmonary tuberculosis (EPTB) received between January 2007 and April 2008. All the specimens were collected with aseptic precautions in sterile leak proof containers and transported to the laboratory. The specimens were processed on the same day for microscopy and culture using standard procedures. [1] Smears were stained with the help of the Ziehl Neelsen (ZN) technique. Specimens were inoculated on Lowenstein Jensen (LJ) media, after decontamination and concentration procedures, and incubated at 37C. The cultures were examined every day for one week and thereafter once a week for eight weeks. Isolates that were obtained within a week were confirmed as acid fast bacilli by the ZN stain. Identification to species level was achieved on the basis of growth on MacConkey's agar, nitrate reduction, and susceptibility to polymixin B 300 units. Minimum inhibitory concentrations (MIC) were determined by broth microdilution using Sensititre CA MHBT (Trek Diagnostic Systems Limited, Imberhorne Lane, East Grindstead, West Sussex RH 19 IQX UK) according to the CLSI guidelines. [3] Inoculum suspensions were prepared by emulsifying three to five colonies in sterile water to a density of 0.5 Mac Farland standard. Fifty microlitres were transferred to a tube of cation adjusted Mueller Hinton broth with TES buffer. One hundred microlitres of this suspension was transferred to each well of the sensititre CA MHBT MIC plate dosed with linezolid, clarithromycin, amikacin, cefoxitin, ceftriaxone, imipenem, minocycline, tobramycin, ciprofloxacin, gatifloxacin, amoxyclav, and trimethoprim sulphamethoxazole in appropriate dilutions. All the wells were covered with adhesive seal and incubated at 30C. Growth appeared as turbidity or as a deposit of cells at the bottom of the well. The susceptible and resistant breakpoints used were those recommended by the CLSI. [3] The disc diffusion method provides a good screening technique for RGM. [4] As the Sensititre CA MHBT had only 12 antimicrobials, susceptibility testing was also carried out on Mueller Hinton agar, using the Kirby Bauer disc diffusion method to the following antibiotic discs supplied by Hi Media Laboratories Pvt. Ltd. A 406 Bhaveshwar Plaza, Mumbai 400086: erythromycin (15 μg), tetracycline (30 μg), vancomycin (30 μg), piperacillin (100 μg), gentamicin (10 μg), and polymixin B (300 units). Results Of the 1062 specimens received for mycobacterial cultures from various clinical specimens from cases of EPTB during the study period from January 2007 to April 2008, 104 (9.79%) grew mycobacteria. Of the 104 mycobacterial isolates, six (5.76%) were rapid growers, which had been obtained from pus and lymph node aspirates. Of these six isolates, three were of M. abscessus, two belonged to M. fortuitum, and one was of M. chelonae. [Table - 1] Shows the MIC breakpoints used for categorization of susceptibility of rapidly growing mycobacteria and the antimicrobial susceptibility of rapidly growing mycobacteria by broth microdilution assay. All three isolates of M. abscessus were resistant to all antibiotics by broth microdilution. However, on a disc diffusion test all showed sensitivity to vancomycin, gentamicin, erythromycin, and piperacillin, and in addition, two showed sensitivity to tetracycline. Of the two isolates of M. fortuitum, one showed sensitivity to all antimicrobials tested by broth microdilution except Imipenem. This isolate was obtained from the pus aspirated from a scapular abscess in a known case of systemic lupus erythematosus (SLE), and the patient had responded to amoxycillin-clavulanic acid. This isolate was also sensitive to vancomycin and gentamicin when tested by the Kirby Bauer disc diffusion test. The other isolate of M. fortuitum was resistant to all antimicrobials by broth microdilution, but was sensitive to tetracycline, vancomycin, and gentamicin. The only isolate of M. chelonae obtained from pus collected from a dental abscess showed intermediate resistance to amikacin (MIC 32 μg/ml) and minocycline (MIC 4 μg/ml) and resistance to all other antibiotics by broth microdilution. This isolate was however sensitive to vancomycin and gentamicin. Discussion Nontuberculous mycobacteria have been reported with varying frequencies worldwide, while in India isolation rates are between 0.7 and 34%. [5] M. fortuitum, M. abscessus, and M. chelonae have been commonly reported to cause skin and soft tissue infections, joint and bursae infections, wound infections, and injection abscesses. In our study RGM constituted 6/104 (5.76%) of all mycobacterial isolates, M. abscessus being the predominant isolate. In a study on nontuberculous mycobacteria isolated from a tertiary care centre in S. India, MV Jesudasan and P Gladstone reported 100 (2.23%) isolates of M. chelonae and M. fortuitum out of 4473 mycobacterial isolates. [6] However, the predominant isolate was M. chelonae. Unlike our study their study had also included pulmonary specimens. Amoxycillin has modest activity against M. fortuitum. Addition of clavulanic acid to amoxycillin enhances the in vitro activity against M. fortuitum. [7] In our study only one isolate of M. fortuitum showed sensitivity to amoxycillin clavulanic acid combination (MIC 4/2 μg/ml). Macrolides and clarithromycin are important agents for treatment of pulmonary and cutaneous infections caused by M. chelonae, M. abscessus, and 80% of M. fortuitum. [2] We observed that only one of the two isolates of M. fortuitum was sensitive to clarithromycin (MIC 0.25 μg/ml), but they were all resistant to erythromycin. All the three isolates of M. abscessus and the only isolate of M. chelonae were resistant to clarithromycin, which has been reported in the past. [8] For oral therapy both sulphonamides and doxycycline were used successfully as single agents in the treatment of cutaneous M. fortuitum infections and erythromycin was used for infections caused by M. chelonae. [7] In our study only one of the two isolates of M. fortuitum was sensitive to trimethroprim sulphamethoxazole (MIC 0.12/2.4 μg/ml). Doxycycline had not been tested. M. chelonae was resistant to erythromycin on disc diffusion test. For serious infections empiric treatment with cefoxitin and amikacin may be started, pending results of susceptibility testing. [7] In our study all the isolates of RGM except one isolate of M. fortuitum were resistant to cefoxitin (MIC > 256 μg/ml) and amikacin (MIC > 128 μG/ml) with the only isolate of M. chelonae showing intermediate resistance to amikacin (MIC 32 μg/ ml). In a study on the sensitivity of rapidly growing mycobacteria, [9] M. chelonae showed resistance to Amikacin (MIC ranging from 1 to 32 μg/ml). Ceftriaxone and anti-pseudomonal penicillins are not known to have significant activity against rapidly growing mycobacteria. [7] None of our isolates, except one, were sensitive to ceftriaxone. However, disc diffusion showed all three isolates of M. abscessus to be sensitive to piperacillin. Tetracycline sensitivity was found to be variable in our study. Three isolates of M. abscessus and one of M. fortuitum were sensitive to it on disc diffusion test. Growth of M. chelonae was slow on Mueller Hinton agar and we repeated the test on blood agar. However, the outer zone margins around tetracycline and erythromycin were not very sharp. A similar problem had been faced by Wallace et al. [4] In the present study all six isolates of rapidly growing mycobacteria were sensitive to vancomycin and gentamicin by disc diffusion test. We had not been able to perform broth microdilution test as it was not included in Sensititre CA MHBT MIC plates. In summary, in the present study M. abscessus and M. chelonae appeared to be resistant organisms, with M. chelonae showing intermediate resistance to amikacin and minocycline. However, all the six isolates showed sensitivity to vancomycin and gentamicin on disc diffusion test. Also all three isolates of M. abscessus were sensitive to pipercillin and erythromycin. Further studies are required to test their sensitivity to these four antimicrobials by using the microbroth dilution test before they can be prescribed to patients when resistance is seen, even to most commonly used antimicrobials such as clarithromycin, amikacin, and cefoxitin. We wish to emphasize that reporting of rapidly growing mycobacteria from clinical settings along with their sensitivity patterns is an absolute need of the hour. Acknowledgement The authors are grateful to Trivitron Diagnostics Pvt Ltd for providing Sensititre CA MHBT for performing MICs of rapidly growing mycobacteria. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10012t1.jpg] |
| |||||||||
{kind=link}