 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
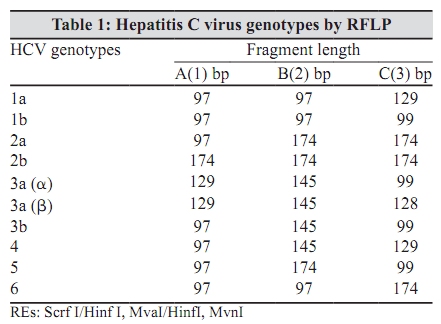
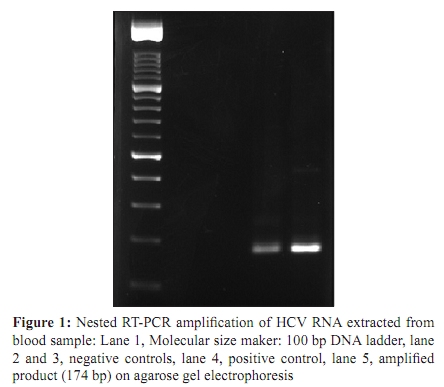
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 54-56 Brief Communication Determination of hepatitis C virus genotypes among blood donors in Ahvaz, Iran *F Farshadpour, M Makvandi, AR Samarbafzadeh, MA Jalalifar Department of Virology, Faculty of Medicine (FF, MM, ARS) and Tropical and Infectious Disease Research Centre, Ahvaz Jondishapour University of Medical Sciences, Golestan Blved, Ahvaz, Ahvaz Blood Transfusion Centre (MAJ), Ahvaz, Iran Correspondence Address: *Department of Virology, Faculty of Medicine (FF, MM, ARS) and Tropical and Infectious Disease Research Centre, Ahvaz Jondishapour University of Medical Sciences, Golestan Blved, Ahvaz, Ahvaz Blood Transfusion Centre (MAJ), Ahvaz, Iran, f.farshadpour@yahoo.com Date of Submission: 22-Apr-2009 Code Number: mb10014 PMID: 20061766 DOI: 10.4103/0255-0857.58731 Abstract This study aims to determine the genotypes of hepatitis C virus (HCV) among blood donors at Ahvaz Blood Transfusion Centre. Blood samples were taken from 2376 blood donors - 1795 (75.54%) male and 581(24.45%) female - who referred to Ahvaz Blood Transfusion Centre during 2007-2008. Detection of anti-HCV antibody for all the donors was carried out by ELISA and the confirmatory RIBA tests. HCV RT-PCR followed by RFLP test was carried out for anti-HCV positive samples. Out of 2376 blood donors, only 55 (2.3%) male donors showed to be positive for HCV antibody by ELISA and RIBA tests out of which 45(1.8%) donors were positive for RT-PCR test. Female donors were negative for HCV antibody. The result of HCV genotyping by RFLP test showed 24 (53.3%) for 1a, 17 (37.7%) for 3a (a) and 4 (8.8%) for 3a (b) genotypes respectively. In conclusion, high prevalence of 53.3% HCV 1a genotype was observed among blood donors in Ahvaz city.Keywords: Blood donors, genotyping, Hepatitis C virus, Restriction Fragment Length Polymorphism, RT-PCR Introduction Hepatitis C virus (HCV) is a single stranded RNA virus which belongs to the Flaviviridae family. [1] HCV is a causative agent for chronic, acute and fulminant hepatitis. [2],[3] The association of HCV among patients with cirrhosis of liver and hepatocellular carcinoma has been reported. [4] HCV infection is a global health problem and it is estimated that 200 million people of the world population are infected with HCV. [5] The study of genetic variability of HCV strains has led the consensus classification into six major genotypes [Table - 1]. [3] Some studies suggest that the clinical features of liver disease depend on HCV genotypes. [6] It is also noteworthy that the success of Interferon and Ribavirin treatment seems to be related to genotypes. [7] Further, HCV genotyping is a useful tool to determine its molecular epidemiology. [2] Ahvaz city is the centre of Khozestan province with a population of about 1.8 million located in the South-West of Iran. There has been no data available so far on HCV genotyping among blood donors in Ahvaz city. This study was conducted to determine HCV genotypes among blood donors in Ahvaz city. Materials and Methods This study, (with research project number U-86069,) was approved by the ethical committee of Ahvaz Jondishapur University of Medical Science. All blood donors gave consent to take part in the experiments voluntarily. The sera were collected from 2376 blood donors referred to the Blood Transfusion Centre from August 2007 to February 2008. The average age was varying from 19 to 50 while the mean age was 34.5. Serological data The sera were collected from these 2376 blood donors. All the sera were initially tested for anti-HCV antibody by Enzyme Linked Immuno sorbent Assay (ELISA) test (Ortho; HCV 3.0 ELISA Test System; Ortho-Clinical Diagnostics, Raritan, NJ, USA). For positive sera by ELISA, the confirmatory Recombinant Immunoblot Assay (RIBA) test (Deciscan; HCV plus; Sanofi Diagnostics Pasteur, SA Marnes la Coquuette, France) was carried out. [2] The positive HCV Ab sera were aliquoted and stored immediately at minus 70°C before use. Extraction of hepatitis C virus RNA We mixed 250 micro litres of serum with 750 ΅l of Trizol LS (Trizol; LS Reagent: Invitrogen, Life Technologies, Carlsbad, CA, USA) for the HCV RNA extraction followed by precipitating by ethanol and then drying. cDNA synthesis HCV-RNA was immediately transcribed into cDNA using random primers (Sensicript RT kit; QIAGEN, Poison Information Centre Mainz, Germany). [8] Hepatitis C virus-RNA detection cDNA was targeted by a nested-PCR directed at the 5' untranslated region using two sets of primers (ROCHE; Roche Diagnostics GmbH, Roche Applied Science, Mannheim, Germany), the first set 5`-AGC GTC TAG CCA TGG CGT -3`, called forward external primer, and 5`- GCA CGG TCT ACG AGA CCT-3`, named reverse external primer. The second set 5`-GTG GTC TGC GGA ACC GG-3`, called forward inner primer, and 5`- GGG CAC TCG CAA GCA CCC-3`, named reverse inner primer of 5'UTR region of HCV genome. The first round was carried out for 30 cycles which consisted of initial denaturation at 94°C for 5 min, denaturation at 94°C for 35sec, annealing at 58°C for 40sec, extension at 72°C for 45sec and, the final extension at 72°C for 5 min. The second round was followed for 25 cycles which consisted of initial denaturation at 94°C for five minutes, denaturation at 94°C for 35 seconds, annealing at 64°C for 40 seconds, extension at 72°C for 45 seconds, and the final extension at 72°C for five minutes. The 174-bp second PCR product was submitted to electrophoresis by using a 1.5% agarose gel in 0.5X TBE buffer, and was visualized by ethidium bromide staining under ultraviolet light. [8],[9] Genotyping The amplicons of each sample were digested by the following three sets of restriction enzymes at 37°C for three hours:
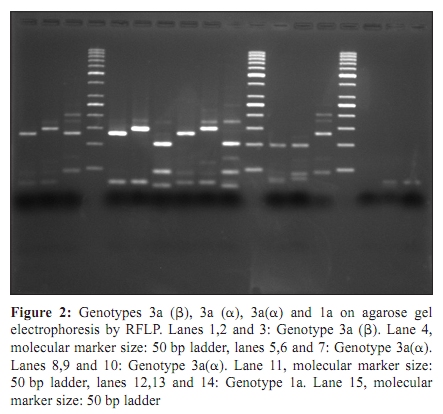
Results Out of 2376 donors, 1795 (75.54%) were males and 581 (24.45%) were females. Of the 2376 blood donors, 55 (2.3%) male donors showed to be positive for HCV antibody while only 45 (1.8%) samples were positive by RT-PCR test. [Figure - 1] shows the 174 bp PCR product. The result of HCV genotyping by RFLP test revealed 24 (53.3%) for 1a, 17 (37.7%) for 3a (a), and 4(8.8%) for 3a (b) genotypes, respectively. [Figure - 2] shows the pattern of RFLP results. Discussion Epidemiological studies in different regions of the world show the wide variation in HCV prevalence patterns [5] though it is clearly revealed that the incidence of HCV is higher among less developed nations. [5] In Iran, HCV prevalence in general population is less than one per cent. [4] In our study, the prevalence of hepatitis C infection was about 2.3% by RIBA and 1.8% by PCR tests, respectively. Regarding the HCV genotypes, 24(53.3%) for 1a, 17 (37.7%) for 3a (a) and 4(8.8%) for 3a (b) genotypes were found among the blood donors. Our results are nearly similar to those studies which have already been conducted by different investigators in Tehran- the capital of Iran. [10],[11] Regarding HCV genotypes, Samimi Rad et al., found 1a (47%), 3a (36%), 1b (8%), and four (seven per cent) genotypes among Iranian patients, and revealed that genotype 1a is frequent in the South of Iran (70%), while 3a is more prevalent in the North-West of Iran (83%). Patients infected by blood products more frequently had genotype 1a (57%), while younger drug users had genotype 3a (54%) more frequently. [10] Keyvani et al., studied distribution frequency of hepatitis C virus genotypes in Iran. In their study, genotype 1a with 39.7% had the highest frequency. Genotype 3a (27.5%) and 1b (12.1%) were the other frequent genotypes. [11] The prevalence of hepatitis C among blood donors is less than one per cent in Northern European countries. [5] Higher rates have been reported in South East Asian countries, including India (1.5%), Malaysia (2.3%), and the Philippines (2.3%). [5] The incidence in Japan is 1.2%. [5] Alarming rates of 14.5% are reported in Egypt. [5] HCV genotype 4 is common in countries such as Yemen, Kuwait, Iraq, and Saudi Arabia. [12] However, genotype 1b is prevalent in Turkey, [12] and HCV genotype 3a is prevalent in Pakistan. [13] Genotype information is important when HCV treatment is being considered, since some genotypes respond more favourably to the medications. Genotype also determines the length of therapy e.g., treatment for genotypes 2 and 3 requires only 24 weeks while genotypes 1 and 4 require 48 weeks. [6] In addition to treatment purposes, detection of HCV genotypes in different regions can be used for the purpose of molecular epidemiology. [6] The results of this study have some similarities with other studies in Pakistan and India, which show that genotype 3 is very prevalent and genotype 2 is very rare. [13] Other studies have shown the absence of genotype 2 in Iran. [13] Conclusion High prevalence of 53.3% 1a genotype and low prevalence of 8.8% 3a (b) HCV genotypes were observed among blood donors in Ahvaz city. Acknowledgments The authors would like to thank Deputy Research and Affairs of Ahvaz Jondishapur University of Medical Science for financial support to meet all expenses and essential equipment for this study. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10014f1.jpg] [mb10014t1.jpg] [mb10014f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}