 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
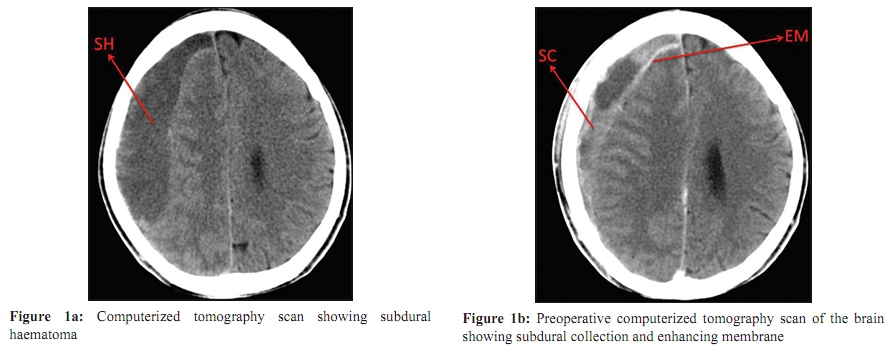
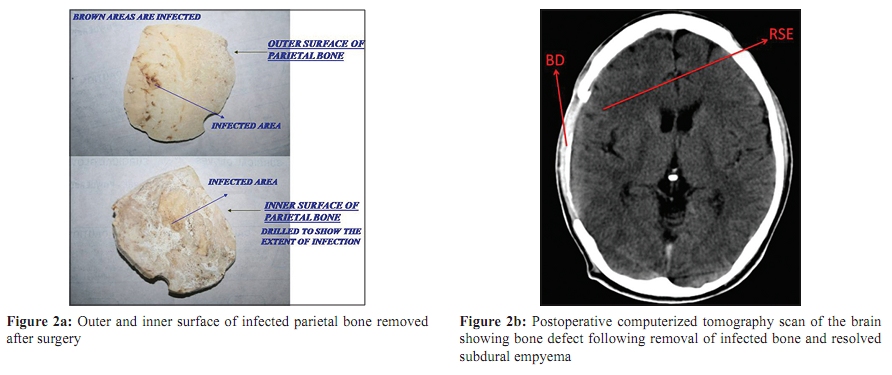
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 60-62 Case Report Chronic subdural empyema and cranial vault osteomyelitis due to Salmonella paratyphi A P Bhooshan, *S Shivaprakasha, KR Dinesh, M Kiran, PMS Karim Department of Microbiology (PB, SS, KRD, PMSK), Department of Neurosurgery (KM), Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala - 682 026, India Correspondence Address: *Department of Microbiology, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala 682 026, India, shashikalapoorna@gmail.com Date of Submission: 25-Jul-2009 Code Number: mb10016 PMID: 20061768 DOI: 10.4103/0255-0857.58733 Abstract Intracranial infections, especially subdural empyema, due to salmonella are rare. Subdural empyema caused by Salmonella paratyphi A has been documented only once earlier in the literature. Hence, we report a case of subdural empyema and osteomyelitis of cranial vault due to S. paratyphi A. A 42- year-old male presented with headache and purulent discharge from right parietal burr hole wound site. Patient gave a history of head injury two years ago. He underwent burr hole evacuation of chronic subdural haematoma, excision of outer membrane and right parietal craniectomy. The cultures grew S. paratyphi A. Recovery was uneventful following surgical intervention and antibiotic therapy. Keywords: Cranial vault osteomyelitis, Salmonella paratyphi A, subdural empyema Introduction Intracranial infections, especially subdural empyema, due to salmonella are rare. Salmonella typhi, Salmonella typhimurium and Salmonella enteritidis have been reported as infecting organisms. [1],[2],[3],[4] Subdural empyema caused by Salmonella paratyphi A has been documented only once earlier in the literature. [1] Salmonella osteomyelitis is a rare entity, constituting 0.8% of all salmonella infections and 0.45% of all types of osteomyelitis. [2] Hence, we report a case of subdural empyema and osteomyelitis of cranial vault due to Salmonella paratyphi A. Case Report A 42-year-old male presented with headache and purulent discharge from right parietal burr hole wound site of two days duration. He was conscious, well oriented and vital signs were normal. There was no neurological focal deficit. Patient gave a history of a head injury in a road accident two years ago and a burr hole evacuation of subdural haematoma done three months later. Subsequently, he underwent evacuation of chronic subdural haematoma [Figure - 1]a through the same burr hole one year and three months later. Computerized tomography (CT) scan done three weeks after the second evacuation revealed the presence of residual subdural haematoma and enhancing membrane [Figure - 1]b. Possibility of infected subdural haematoma was suspected. He then underwent re-exploration, evacuation of subdural empyema, excision of outer membrane and removal of infected right parietal bone [Figure - 2]a. Aspirated pus and parietal bone cultures grew Salmonella paratyphi A. Gram stain of the aspirated pus revealed the presence of gram negative bacilli. The samples were inoculated on MacConkey agar, sheep blood agar and growth was observed after 16-18 hours of incubation at 37ΊC. On MacConkey agar, colonies were non lactose fermenting, low convex, and smooth. On sheep blood agar colonies were greyish and non haemolytic. The isolated organism was identified as Salmonella paratyphi A based on biochemical reactions and by using specific antisera [Salmonella O (A-E) and Salmonella paratyphi AH]. [5] The laboratory investigations revealed total leukocyte count 12.1 K uL (4.4-11.3), neutrophils 90.4% (37.0-80.0), lymphocytes 8.24% (10.0-50.0), erythrocyte count 3.97M/uL (4.5-5.9), haemoglobin 11.1g/dl (14.0-17.4), platelet count 428.0 K/uL (150.0-450.0). Antibiotic susceptibility testing was done on Mueller-Hinton agar by modified Kirby Bauer technique as described by the Clinical and Laboratory Standards Institute (CLSI). [6] The isolates were sensitive to ampicillin, ciprofloxacin, chloramphenicol, cotrimoxazole and ceftriaxone. Patient was treated with ciprofloxacin for 15 days and parenteral chloramphenicol for 10 days initially. Ciprofloxacin was continued for another four weeks and cotrimoxazole was administered for four weeks. As expected, widal test done during the follow-up visit showed significant titre (O-40 and AH-320). Recovery was uneventful following surgical intervention along with antibiotic therapy and CT scan done at that time showed resolved subdural empyema [Figure - 2]b. He was followed up at regular intervals and at the end of one year period he was normal. Discussion Subdural empyema is the second most common type of intracranial bacterial infection. The subdural space is between the two outer layers of the meninges - dura mater and arachnoid mater. There is a large potential space for pus to spread through with only a few anatomical restrictions. Thus, subdural empyemas behave as rapidly expanding space-occupying lesions. It frequently occurs in the left frontoparietal region. Left undiagnosed and untreated, subdural empyema is rapidly fatal, and hence early recognition is critical. Subdural empyema may occur at any age, but is most commonly seen in the second and third decades of life. Men are four times more commonly affected than women. [7],[8] The organisms recovered most often from subdural infections are aerobic and anaerobic streptococci. Staphylococci are cultured less frequently, followed by aerobic gram negative bacilli and non streptococcal anaerobic cocci. Other organisms reported to cause subdural empyema are Salmonella spp., Campylobacter foetus, Serratia marcescens, Neisseria meningitidis, Pasteurella multocida, Actinomyces israelii, and Actinobacillus actinomycetemcomitans. [8] The types of bacteria grown will reflect the predisposing source. The probable pathogens causing subdural empyema after cranial surgery or trauma include Staphylococcus aureus, coagulase negative staphylococci, Clostridium spp., Enterobacteriaceae, and Propionibacterium acnes. Subdural empyema with Salmonella spp. have been reported in neonates and infants after the occurrence of meningitis. Clinically, an infected subdural haematoma manifests with non-specific signs of infection, focal neurological signs and signs of increased intracranial pressure. In most patients, fever and headache precede a fulminant loss of conciousness. [7],[9] Predisposing factors for salmonella osteomyelitis include sickle cell anaemia, systemic lupus erythematosus (SLE), haematological neoplasm, immunosuppressive therapy, and impaired cell mediated immune response. In less than 1% of cases it occurs as complication of enteric fever. [10] In this case, probable predisposing factors for osteomyelitis are cranial surgery and underlying subdural empyema. To summarise, the three basic principles for the prompt and effective treatment of cranial subdural empyema are early removal of source of infection, drainage of subdural pus and use of appropriate antibiotic medications. [1] We emphasize, that in a case of chronic subdural haematoma, the possibility of an infective cause should be borne in mind and investigated appropriately for optimal treatment. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10016f2.jpg] [mb10016f1.jpg] |
| |||||||||

{kind=link}
{kind=link}