 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
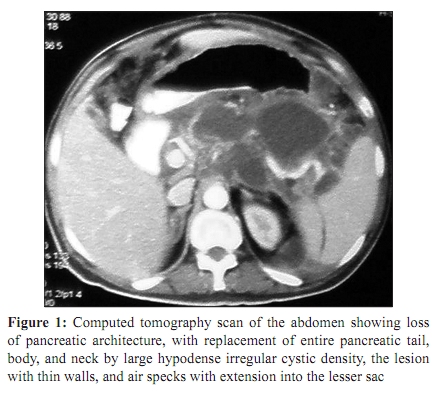
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 64-67 Case Report Acute necrotizing pancreatitis with pancreatic abscess due to Prevotella species in a diabetic A Sonavane, *V Baradkar, P Salunkhe, D D’Souza, S Kumar Department of Microbiology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai - 400 022, India Correspondence Address: *Department of Microbiology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai - 400 022, India, vasantbaradkar@yahoo.com Date of Submission: 17-Jan-2009 Code Number: mb10018 PMID: 20061770 DOI: 10.4103/0255-0857.58735 Abstract Acute pancreatitis occasionally presents as pancreatic abscess with complications like pleural effusion and ascites. There are several pre-disposing factors, the most common being cholelithiaisis, alcohol abuse, infective causes, trauma, and metabolic causes such as diabetic ketoacidosis, while some cases are idiopathic. Here, we report a rare case of acute necrotizing pancreatitis in a 40-year-old male who presented with pain in the abdomen, ascites and left basal pleural effusion. A computerized tomography (CT) scan showed findings suggestive of pancreatic necrosis, with abscess formation and free-fluid surrounding area. The aspirated pus sample was processed for Gram staining and culture, which yielded growth of Prevotella species in an anaerobic culture. Exploratory laparotomy was performed and intra-abdominal collection drained. Necrosectomy of the distal tail and body of the pancreas was performed. The patient was started on antibiotics and along with supportive treatment, responded well.Keywords: Diabetes, pancreatic abscess, Prevotella species Introduction The Atlanta Conference, [1] in 1992, defined pancreatic necrosis as diffuse or focal area(s) of non-viable pancreatic parenchyma typically associated with peripancreatic fat necrosis. The necrosis is either sterile or infected depending on the presence of infection. The morbidity and mortality associated with acute pancreatitis are substantially higher when necrosis is present, especially in cases when the necrotic area becomes infected. [2],[3] There are several cases of pancreatitis, which include cholelithiaisis, ethanol abuse, diabetes mellitus, trauma, ischaemia due to other causes, drugs, penetrating duodenal ulcer, and some cases being idiopathic. [2],[3] Nearly 25% of all attacks of pancreatitis have severe complications and the death rate of clearly diagnosed cases has remained high, at 10-25%. Most studies on acute pancreatitis are based on the Western population. [4] It is generally perceived that acute pancreatitis runs a benign course in Asian countries and that the aetiology is different from that of the Western population. [4] Severe disease is characterized by organ failure and/or local estimate. Around 20-30% of all patients will have a severe clinical course of the complications such as necrosis, pseudocyst, or abscess and 95% of the deaths will occur in this subset. It is generally reported that the overall mortality of acute pancreatitis is 5-10% and may increase to 35% or higher if complications develop. [4] We report a rare case of necrotizing pancreatitis with pancreatic abscess due to an anaerobe, Prevotella species, in a diabetic patient, who responded to treatment. Case Report A 40-year-old male was admitted with severe pain in the abdomen on December 27, 2007 The patient was a known case of diabetes on insulin therapy and also a chronic alcoholic. A CT scan of the abdomen showed findings suggestive of acute necrotizing pancreatitis and investigations revealed that he was also in diabetic ketoacidosis. His hemoglobin was 8.4 g/dl, total leukocyte count was 16,000/ mm 3 , with a differential count of 80% polymorphs and 20% lymphocytes, blood urea nitrogen was 10 mg%, serum Na+ level was 138 meq/l, K+ was 2.4 meq/l, Ca 2+ was 7.8 meq/l, adenosine deaminase level was elevated, and serum lipase level was 346.74 U/l. The chest X-ray showed left-sided pleural effusion. Ascitic fluid and pleural fluid tapping was performed. About 450 milliliters of pleural fluid was tapped from the left pleural cavity for bacteriological culture, which did not yield the growth of any organism. The patient was administered Ofloxacin 400 mg twice, daily, and insulin and pancreatic enzymes to which he responded well. He was discharged on January 23, 2008. The patient was re-admitted on February 4, 2008, with complaints of abdominal pain and abdominal distension. He gave a history of having stopped insulin 10 days before the presentation of symptoms. On examination, the patient was afebrile, with a pulse rate of 92/min and a blood pressure of 120/80 mmHg. There was mild pallor noted but no icterus. The findings of the cardiovascular system were within normal limits. On auscultation, crepitations were observed at the base of the left lung. Per-abdominal examination revealed moderate ascites. Investigations revealed that he had a hemoglobin of 10 g/dl, total white blood cell count of 18,400, with 98% neutrophils and two per cent lymphocytes, and blood sugar levels of 350 mg/dl. The serum lipase was 310 IU/l and the serum amylase was 330 IU/l. The CT scan [Figure - 1] showed findings suggestive of acute necrotizing pancreatitis with multiple phlegmatous thin wall collection. Exploratory laparotomy showed approximately three to five liters of muddy purulent intra-abdominal collection tracking to the anterior abdominal wall, retro peritoneum, and pancreatic gutter. There was necrosis of the body and tail of the pancreas. The fluid was collected under aseptic precautions and was cultured for aerobic and anaerobic organisms. The Gram-stained smear showed presence of pus cells with Gram negative bacilli. The aerobic culture did not yield any bacterial growth whereas on anaerobic Blood agar, there was growth. The gram stained smear from the colony showing coccoid gram-negative rods [Figure - 2] which was further identified to be Prevotella species by standard laboratory procedures. [1] Intra-abdominal collection was drained and necrosectomy of the distal tail and body of the pancreas was performed. The patient was given Piperacillin plus Tazobactam along with Metronidazole intravenously. The patient was discharged after a period of three weeks, with controlled blood sugar levels and signs of improvement and fall in the serum lipase and amylase levels. The patient was asked to have check ups in the outpatient department at regular intervals. The first check up showed that the patient was doing well, with no signs of deterioration and normal serum lipase and amylase levels. Discussion Acute pancreatitis is defined as an acute inflammatory process of the pancreas, with variable involvement of other regional tissues or remote organ systems. [2],[3],[4] Acute pancreatitis is classified as either mild (85% of cases) or severe (15% of cases). Mild acute pancreatitis is a self-limiting disease associated with minimal organ dysfunction and characterized by scattered areas of fat necrosis, oedema, and acute fluid collection (i.e., collection of fluid that lack a wall of granulation tissue or fibrous tissue). [2],[3],[4] Severe acute pancreatitis is associated with organ failure or local complications such as necrosis, abscess, and pseudo cyst and is often characterized by extensive peripancreatic fat necrosis, parenchymal necrosis, and hemorrhage. It usually declares itself shortly after the onset of abdominal pain, and delayed progression from mild acute pancreatitis to severe acute pancreatitis is rare, as happened in the present case. [2],[3],[4] Although much has been known regarding the risk factors, pathology, and biochemical events, the exact trigger event or pathogenesis still remains elusive. [3] Predisposing factor-associated pancreatitis include cholelithiaisis, ethanol abuse, idiopathic causes, metabolic causes like diabetes ketoacidosis, hypercalcaemia, uremia, trauma (post-operative or blunt abdominal), organophosphorus poisoning, penetrating duodenal ulcer, drugs like thiazides, oral contraceptives, tetracycline, and pentamidine, and infections due to mumps, Coxsackie A and B, mycoplasma, viral hepatitis (A, B, and C), cytomegaolvirus, varicella, Ebstein-Barr virus, adenovirus, leptospirosis, and Mycobacterium tuberculosis. In the present case, two predisposing factors were obvious, i.e. diabetic ketoacidosis and alcohol abuse. In severe acute pancreatitis, patients frequently develop a pancreatic inflammatory mass within 2-4 weeks. There may be extended areas of necrosis in some cases. [2],[ 3] Complications associated with pancreatitis include local complications like pancreatic necrosis, abscess, pseudo cyst, ascites, retoperitoneal haemorrhages, venous (splenic, renal, or portal vein) thrombosis, or systemic, like pulmonary effusions, acute respiratory distress syndrome, mediastinal abscess, disseminated intra-vascular coagulation, acute renal failure, peptic ulceration, acute stress ulceration, and central nervous system complications like encephalopathy, seizures, psychosis, and sudden blindness. In the present case, there was associated pancreatic necrosis and abscess along with pulmonary complications, i.e. left-sided pleural effusion. The clinical presentation in pancreatitis may vary. Epigastric abdominal pain, which may radiate to the back, chest, or lower abdomen, is the predominant symptom of acute pancreatitis, which was present in the case. Nausea and vomiting may occur in up to 90% of the cases. Abdominal signs of tenderness, rigidity, guarding, and distension and respiratory signs of pleural effusion, basal collapse, wheezing, and basal crepitations are found in 10- 20% of the cases. In the present case, there were abdominal signs and left-sided pleural effusion with basal crepitations, but other signs such as Cullen's sign or Grey-Turner's sign which might be observed in some cases were not found. The diagnosis of severe acute pancreatitis was based on the conglomeration of clinical picture, biochemical parameters, and imaging modalities. The marked elevation of serum amylase levels in acute pancreatitis, as observed in the present case, along with the raised serum lipase levels, has a specificity of almost 90%. [2],[3],[4] The complete blood picture, with leukocytosis above 15,000/mm 3 and hematocrit of more than 50% (due to loss of plasma), are commonly found in severe acute pancreatitis. CT scan is the "gold standard" for diagnosing pancreatic necrosis and peripancreatic collections. [5] It offers an opportunity to reliably determine both the presence and the extent of pancreatic fatty tissue necrosis with an accuracy of more than 90% when there is more than 30% glandular necrosis. [5] About 30% of the patients with severe acute pancreatitis develop infection. [6],[7] Most of these infections are due to enteric organisms like Escherichia coli, Klebsiella pneumoniae, Enterococcus species, Pseudomonas aeruginosa, Staphylococcus aureus, and Mycobacterium tuberculosis. [6],[7] Anaerobic organisms are known to cause intra-abdominal infections and other deep-seated infections. [8],[9],[10] These anaerobes include Peptostreptococcus species, Bacteroides fragilis, Prevotella species, Porphyromonas species, Clostridium species, and Fusobacteria. [8],[9],[10] Brook et al., [10] in 1998, reviewed 161 cases of retroperitoneal abscesses, of which 109 were anterior, eight posterior, 21 retrofascial, and 23 pelvic abscesses. Of the 109 anterior retroperitoneal abscesses, 46 were cases of pancreatic abscesses. Pre-dominant anaerobic organisms reported in that study include Peptostreptococcus species (95), Bacteroides species (66), Prevotella species (22), and Clostridium species (22). In the present case, Prevotella species was responsible for the secondary infection, which was amenable to treatment with antibiotics. Specific treatment for acute pancreatitis currently does not exist and management is still supportive, administration of fluid, electrolytes, providing pain relief, and to prevent complications. The only absolute indication for surgery in necrotizing pancreatitis is the confirmation of infection in necrotic pancreas and surrounding tissues and aspiration of necrotic material and fluid collection around the pancreas. Infected cases require laparotomy and surgical drainage (necrosectomy) along with antibiotics. [2],[3],[4],[5] Conclusion Pancreatic necrosis is being increasingly recognized as a complication of severe acute pancreatitis. [2],[3],[4] The clinician who makes the initial assessment needs to have a very high index of suspicion, as early institution of supportive therapy, followed by other modalities of treatment to reduce morbidity and mortality, which may otherwise be as high as 80%, References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10018f1.jpg] [mb10018f2.jpg] |
| |||||||||
{kind=link}
{kind=link}