 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 67-71 Case Report Acanthamoeba keratitis with Curvularia co-infection *N Gupta, JC Samantaray, S Duggal, V Srivastava, CS Dhull, U Chaudhary Zoonotic Division (NG), National Institute of Communicable Diseases, New Delhi, India; Department of Microbiology (JCS), All India Institute of Medical Sciences, New Delhi, India. Department of Microbiology (SD), BL Kapur Memorial Hospital, Pusa Road, New Delhi, India; Department of Microbiology (VS), Sahara Hospital, Lucknow, Uttar Pradesh, India; Department of Ophthalmology (CSD), Department of Microbiology (UC), Pt. B. D. Sharma Post Graduate Institute of Medical Sciences, Rohtak, Haryana, India. Correspondence Address: *Zoonotic Division (NG), National Institute of Communicable Diseases, New Delhi, India, naveen7420625@yahoo.com Date of Submission: 20-Feb-2009 Code Number: mb10019 PMID: 20061771 DOI: 10.4103/0255-0857.58736 Abstract We report a case of Acanthamoeba keratitis with Curvularia co-infection. Acanthamoeba and fungal co-infection have been uncommonly reported in literature, worldwide. A classical history with a strong clinical suspicion and experienced laboratory personnel with systematic examination of corneal scrapings for bacterial, viral, parasitic and fungal causes are imperative for accurate diagnosis. Early diagnosis of Acanthamoeba keratitis or fungal infection followed by aggressive and appropriate treatment with effective agents is critical for the retention of good vision. Acanthamoeba keratitis is difficult to diagnose and, despite improvement in treatment options, may culminate in prolonged morbidity and significant loss of visual acuity. This case emphasizes the important role played by clinical microbiologists in making prompt diagnosis which can ultimately reduce visual morbidity.Keywords: Acanthamoeba, curvularia, keratitis Introduction Microbial keratitis has been reported to be due to infection with a wide range of organisms. There are regional variations in the predominance of different microbes, reflecting different patient population and climatic effects. [1] Fungi are important in the tropical region whereas Acanthamoeba has been identified among contact lens related infections in many parts of the world. [2] Acanthamoeba keratitis continues to be a cause of concern to the ophthalmologist. Although specific clinical features have been described for bacterial, fungal and parasitic corneal infection, prolonged use of wrongly administered antimicrobial agent and/or corticosteroids and patient or parasite related factors could result in a considerable overlap of the identifying features. [2] Definite diagnosis of keratitis depends on the results of laboratory examination. Only sporadic cases of Acanthamoeba keratitis have been reported, despite the worldwide existence of this organism in the environment. Possible reasons for this low incidence include a lack of awareness by physician and inadequate facilities for laboratory diagnosis. [3] Early diagnosis of Acanthamoeba keratitis and successful medical treatment, gives a better visual prognosis. However, poor final out come in many studies are related to delayed diagnosis, central scar, glaucoma, drug resistance of the organisms, and microbial co-infection. [4] Mycotic keratitis may occur at any age, but the highest incidence coincides with the period of maximal activity. [5] Men are involved twice as often as women and agricultural workers and outdoor labourers constitute the biggest occupational group. Minor injury to the eye is an important pre-disposing factor. [5] Aspergillus accounts for nearly 50% of the reported cases of mycotic keratitis and is the most frequent fungus in many parts of India. [6] Fusarium [7] and Candida[6] are considered the most common causes elsewhere. Of dematiaceous fungi, Curvularia has been most often been involved in mycotic keratitis. [8] This emphasizes the importance of prompt diagnosis in recognizing and identifying fungal/Acanthamoeba infection as antifungal/anti amoebic agents will minimize visual morbidity. Case Report A 39-year-old male, shopkeeper by occupation, presented with pain in the left eye for one month; redness, photophobia, watering and lid swelling for 15 days and diminution of vision for 10 days. The patient gave history of removal 'foreign body cornea' left eye by an eye specialist one month ago and administration of ciprofloxacin eye drops. However, pain continued and other symptoms like redness, photophobia, watering and lid swelling developed. The patient consulted for the second time and was prescribed lomefloxacin, tobramycin, natamycin and cyclopentolate eye drops. A few days later, his complaints progressed further with diminution of vision. Finally, he presented in ophthalmology OPD of our hospital. There was no history of injury to the left eye or of contact lenses and no prior history of intermittent attacks of pain, redness or diminished vision in either eye. However, there was history of swimming in a pond one month back. On examination, vision in right eye was 6/6 (normal). In left eye, it was restricted to hand movements and finger counting. Eyebrows, orbital margins and wrinkling of forehead were normal. In the left eye, eye ball, lachrymal apparatus, iris, pupil and intraocular pressure were normal. Both upper and lower lids were swollen and warm on palpation and vertical palpebral aperture was decreased (two mm). Superficial and deep congestion was present in the conjunctiva with formed anterior chamber, normal in depth and small keratic precipitates at the back of cornea. The cornea was:
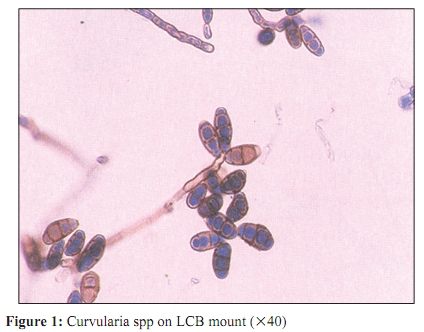
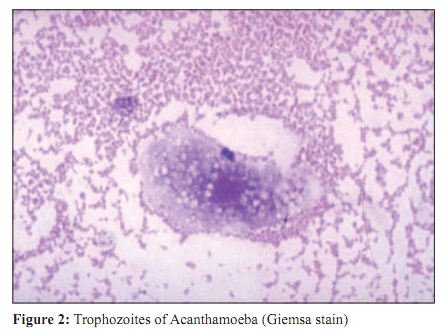
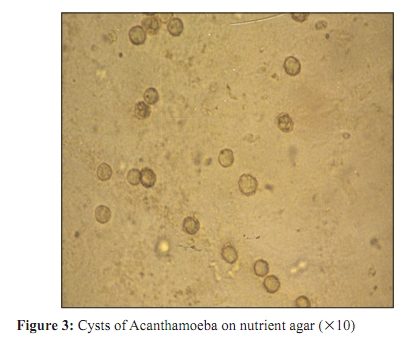
Clinically, the diagnosis of Acanthamoeba -herpetic, fungal or bacterial corneal ulcer was made. The ophthalmologist collected corneal scrapings in the microbiology laboratory and directly inoculated them onto culture media (blood agar, chocolate agar, Saboraud's dextrose agar (SDA) and nutrient agar with lawn culture of Escherichia coli) and on a slide for microbiological examination. Due to scarce material available, direct microscopy was unyielding. After 24 hours of incubation at 37C all the media were sterile SDA and nutrient agar were further incubated at 37C and examined daily for the growth of fungus and Acanthamoeba respectively. On day 4, dematiaceous fungus was isolated on SDA, later identified as Curvularia spp. by slide culture [Figure - 1]. On day 5 a small zone of clearing of E. coli lawn culture was observed around the area of inoculation of corneal scraping. A wet mount was prepared from the edge which showed 15-30 μ sized trophozoites with spiny pseudo pods, with prominent nucleus and vacuole and sluggish motility. The Giemsa stain also showed clear cut morphology of the trophozoites [Figure - 2]. The nutrient agar culture plate was examined under 10x of light microscope which revealed trails of the organism and the dividing trophozoites while the zone of clearing showed round cysts which were double walled with polyhedral inner cyst wall [Figure - 3]. The culture plate was incubated for further 24 hours, zone of E. coli clearing progressed and the number of cysts increased markedly. A provisional diagnosis of Acanthamoeba and Curvularia keratitis was done and patient was put on one per cent propamidine isothionate, natamycin, fluconazole, neosporin and cycloplegic eye drops. Other supportive treatment included analgesics and multivitamins. The isolate on the nutrient agar was processed further and a 1 cm x 1 cm agar block subculture, from the zone of clearing, was done on non-nutrient agar, nutrient agar and five per cent sheep blood agar, all with E. coli lawn cultures. Within 48 hours all, the three media showed the presence of Acanthamoeba. However, gross zone of clearing was better appreciated on nutrient agar with E. coli. The trails of Acanthamoeba were well appreciated on all the three media. The growth of amoeba on non nutrient agar ruled out Balamuthia spp. the amoeba could grow at 40°C and did not convert to flagellate form in distilled water (ruled out Naegleria fowleri). After a week of therapy, inflammation, discharge and swelling decreased markedly. Further progression of lesion stopped and pain in the eye decreased considerably. The patient was managed conservatively and discharged as his vision improved and active infection stopped. Discussion Acanthamoeba spp. is an opportunistic pathogen that produces multifocal encephalitis called granulomatous amoebic meningoencephalitis (GAE) and various other disease states including keratitis and pneumonitis. [9] A. castellani, A. culbertsoni and A. polyphaga are the most commonly associated with keratitis and GAE. [9] Acanthamoeba spp. pervade the entire environment and can be found in tap, fresh, coastal and bottled mineral water, sewage, contact lens solutions and eyewash stations, soil, dust and air, heating, ventilation or air conditioning units, dialysis machines and dental units, hot tubs, and gastrointestinal washings. [9] Most episodes of keratitis occur during warm weather and often follow water exposure or a history of swimming in lakes and ponds while wearing contact lenses. [9] A classical history with a strong clinical suspicion often helps in narrowing the diagnosis and selecting therapy. Common diagnostic criteria include unilateral infection, history of prior minor corneal trauma, or exposure to soil or standing water. [10] Clinical characteristics include repeated epithelium erosion, infiltrative (often ring shaped) stromal keratitis, scleritis, variable uveitis, severe ocular pain sometimes requiring narcotics, standard bacterial culture negativity chronicity, and lack of response to antimicrobial agents. Experienced laboratory personnel; whether ophthalmic pathologist or microbiologist; should be alerted to the possibility of Acanthamoeba infection. Microbiologic strains, media and immunofluorescence are imperative for accurate diagnosis. The advent of confocal biomicroscopy has permitted detection of Acanthamoeba by polymerase chain reaction diagnostic technique. [11] It is now appreciated that early diagnosis of Acanthamoeba keratitis is critical for the retention of good vision. Bacon and co-authors reported that the infection is misdiagnosed as herpes simplex keratitis in 11% of patients. [12] Herpetic keratitis usually presents with frank ulceration of the corneal epithelium, while amoebic keratitis causes an oedematous and necrotic appearance of the involved epithelium. Dendritiform keratitis is a major feature of Acanthamoeba keratitis. [13] The characteristic double walled cysts seen on smears of corneal scrapes stained with Gram's or Giemsa establish the early tentative diagnosis. [14] Confocal microscopy and other methods such as indirect immunofluorescence also allow early diagnosis. [15],[16] Diagnosis within one month of symptoms and institution of early treatment are associated with excellent visual outcome. [17] Treating keratitis with a combination of amoebicidal agents can have a favourable outcome. Cationic antiseptics such as polyhexamethylene biguanide (PHMB) and chlorhexidine digluconide, which interfere with membrane function, can be use in conjunction with aromatic diamidines such as hexamidine, pentamidine and propamidine isothionate, which inhibit DNA synthesis to provide maximal primary coverage. [18] PHMB has been successfully used in combined treatment with propamidine and neomycin but commercial eye drop preparations are not available. Successful surgical treatment includes epithelial debridement and keratoplasty, but these are complicated by recurrent infections in 30% of grafts, secondary glaucoma, and graft failure. [19],[20] Thus, successful therapy (or both) directed at killing the cyst in the tissue or removing the infected tissue and preventing secondary bacterial infection. Acanthamoeba keratitis can be a devastating infection in the following situations:
Injudicious use of topical corticosteroids and antibacterial agents for external ocular diseases enhances the risk of fungal corneal ulcer. [22] Curvularia infection is usually acquired by direct inoculation or inhalation. [23] Keratitis due to filamentous fungi is believed to usually occur following trauma, the key disposing factor, in healthy young males engaged in agricultural or other outdoor work; traumatizing agents of plant or animal origin (even dust particles) either directly implant fungal conidia in the corneal stroma or abrade the epithelium, permitting invasion by exogenous fungi. Less frequent factors include immunological incompetence, prior administration of corticosteroids or antibacterial agents, allergic conjunctivitis and the use of hydrophilic contact lenses. [24] Trauma was the most common predisposing factor (55.3%) followed by associated systemic illness (11.2%), previous ocular surgery (9.8%) and others. [25] In another study, corneal injury contaminated with vegetable matter was responsible for 60.5% of traumatic cases. [26] Aspergillus spp were the most common isolates (39.5%) in Mycotic keratitis followed by Fusarium (10.7%), Alternaria (10.2%), Curvularia (7.4%) and Penicillium (7%). [25] There are other some reports that Fusarium (37.2%) and Aspergillus species (30.7%) predominated the hyaline fungal spectrum and Curvularia spp were the highest among the dematiaceous fungal keratitis isolates. Of 360 cases of clinically suspected suppurative keratitis, amongst positive isolates, 79% were bacterial and 16% fungal (predominantly Candida albicans) and protozoal (Acanthamoeba), according to an Australian study. [27] The management of Curvularia infections usually involves surgical treatment with or without the use of antifungal drugs. Some patients have been successfully treated with amphotericin B. Despite their in vitro efficacy, therapy with azoles such as miconazole and ketoconazole has been disappointing due to the frequent recurrence of infection. Itraconazole and terbinafine have also been used successfully for localized infections; surgical treatment alone may also be adequate. [23] Such corneal microbial co infections pose a challenge to the ophthalmologist because of its tendency to mimic other types of stromal inflammation and because its management is restricted by the availability of effective antifungal and anti amoebic agents and the extent to which they can penetrate into the corneal tissue. In this particular case, direct microscopy was unyielding and maximum material was used for culture using standard techniques to establish Acanthamoeba, bacterial or fungal diagnosis. Evidences that both the agents, isolated Acanthamoeba and Curvularia, were pathogens and not environmental contaminants are:
Conclusion When Acanthamoeba keratitis is severe, it is relatively easy to diagnose microbiologically by culture. Culture positive disease may be the tip of the iceberg. Therefore, a simple and easy method to culture Acanthamoeba is strongly desired. The nutrient agar and any strain of E. coli are routinely available in any microbiology laboratory. Therefore, for the initial isolation of the free living amoeba on nutrient agar with E. coli lawn culture may be used. Also, with this method the results are quick and easy to interpret and can be confirmed with the help of various other specific tests. Only a few cases of combined fungal and Acanthamoeba keratitis have been described in the literature. The ultimate response of the patient to therapy is directly related to the severity of infection at the time of diagnosis and initial single or multidrug therapy. Ultimately, Acanthamoeba keratitis may be fairly common or relatively rare; it is blinding illness that is potentially curable. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10019f3.jpg] [mb10019f2.jpg] [mb10019f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}