 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
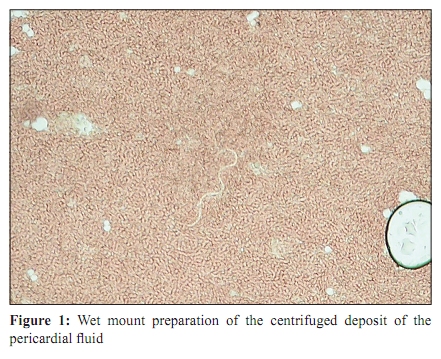
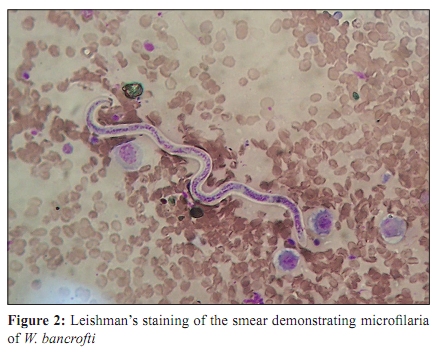
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 73-75 Case Report Unresolving pericarditis: Suspect filariasis in the tropics *K Prasanthi, K Nagamani, NK Saxena Department of Microbiology, Gandhi Medical College, Secunderabad - 500 003, India Correspondence Address: * Department of Microbiology, Gandhi Medical College, Secunderabad - 500 003, India, bebold_p@yahoo.co.in Date of Submission: 10-Dec-2008 Code Number: mb10021 PMID: 20061773 DOI: 10.4103/0255-0857.58738 Abstract Filariasis, a mosquito-borne disease, is wide spread in India. While laboratory diagnosis has been conventionally done by demonstrating microfilaria in peripheral blood smears, occasionally they are reported in various body fluids including pericardial fluid. We report the case of 33-year-old man with severe dyspnoea and chest pain, referred from a private nursing home with a provisional diagnosis of unresolving pericarditis. Pericardial tap revealed massive pericardial effusion with actively motile microfilariae. No microfilariae (Mf) were seen in the peripheral blood. Haemorrhagic effusion resolved completely with DEC. Though relatively uncommon, tropical diseases must always be considered in the etiological diagnosis of pericardial effusion.Keywords: Filariasis, microfilaria, peircardial effusion Introduction Nearly one-third of the world's population, at risk of lymphatic filariasis, live in India. Of these, 98% are caused by Wuchareria bancrofti. Common clinical manifestations are due to inflammatory reactions of lymphatic system, sequelae of their obstruction or fibrosis and rupture. Demonstration of microfilariae in the peripheral blood smear or in the tissues is the mainstay of diagnosis. The Mf are not just confined to the lymphatic system but also associated with other organs, tissues and serous cavities like pleura, pericardium etc. [1] Though reporting of filarial intrusion in aberrant sites especially pericardium has increased, the paucity regarding these type of cases still exists, probably due to lack of realization of this condition as one of the important causes of pericarditis in the tropics. The first case of filarial pericardial effusion was reported in the year 1963 by Mukherji et al, [2] second case was by Chakravarty et al. in 1966, [3] and third, fourth cases were by Sinha et al. in 1971, [4] Samantaray et al.1975 [5] respectively. Subsequently, very few cases were reported on filarial intrusion, in aberrant sites, especially pericardium. Diagnosis of pericardial effusion is incomplete unless the etiology is determined and expressed. Though relatively uncommon, tropical diseases must always be considered in the etiological diagnosis of pericardial effusion. Case Report A 33 year old male patient was referred from a private hospital of Bidar district, Karnataka with a provisional diagnosis of massive pericardial effusion and cardiac tamponade. The patient was brought to casuality with severe breathlessness, chest pain and fever. On examination he was severely dyspnoeic, emaciated and weak with moderately enlarged, firm cevical lymphadenopathy on right side of neck and mild Hepatomegaly. Heart sounds were muffled. He was admitted to the Cardiology ICU and was treated with Cefotaxime and Metronidazole with supportive therapy. The patient had similar complaints for the past one month for which he was admitted, investigated and treated in a private hospital, where pericardial tap was done twice. With the recurrence of pericardial effusion and persistant dyspnoea, patient was referred to Gandhi hospital, Secunderabad.The patient was not a diabetic, hypertensive or a smoker, but alcoholic. No previous history of Tuberculosis, Rheumatic fever, Filarial infection or Malignancy could be elicited. Various investigations were done. Results were as follows Complete blood picture (CBP)- Total count - 7100, polymorphs - 68, lymphocytes -28, eosinophils - 02, monocytes - 02, platelet count-1.5, haemoglobin-11 gms, ESR-42 1Hr, absolute eosinophilic count (AEC) - 216cells/cumm, HIV-non- reactive, HBsAg-negative, adenosine deaminase(ADA)-38 units/L, complete urine examination(CUE)-normal, blood sugar, urea, creatinine, electrolytes all were in normal range. Fine needle aspiration cytology of enlarged cervical lymphnode was done to rule out filarial or tuberculous etiology. X ray, ECG and Echo revealed massive pericardial effusion. Pericardiocentisis was done and 1250 ml of haemorrhagic fluid was collected. A continuous drain was arranged. Cytological analysis of fluid showed-400 cells/ cmm, (neutrophils-20%, lymphocytes-50%, reactive mesothelial cells-30%, plenty of RBC), negative for malignant cells, sugar-49 mg/dl, proteins-4.9 gm/dl. AFB-negative; microscopy and routine cultures were negative for bacteria. While screening the smears, a few large, long, smooth walled, refractile unstained worm like structures were observed. Wet mount examination of centrifuged deposit revealed several long actively motile forms [Figure - 1]. The organisms were identified as Microfilariae of Wuchareria bancrofti in the smears stained by Leishman's stain [Figure - 2]. Peripheral blood smears were negative for microfilariae. DEC provocation test was negative. Patient was started on diethylcarbamazine (DEC) 100 mg thrice a day immediately. The patient was rapidly improved by next day and effusion was grossly reduced by the third day and the drain was removed. DEC was continued for three weeks. The cardiac silhouette returned to normal. FNAC report of cervical lymphnode revealed secondary Metastatic deposits. For confirmation FNAC was repeated. Later, patient was referred to MNJ cancer institute, Hyderabad, for further treatment. Discussion The present case was of huge pericardial effusion established as filarial in origin on demonstration of Mf in pericardial aspirate. The patient did not have any other evident features of filariasis. Usually chylous serous effusions are well established manifestations of filariasis. This case had haemorrhagic effusion which otherwise favored the diagnosis of malignant effusion. From this stand point, either the biology of the worm or the pathogenesis of the disease, filariasis probably is the least well understood of all helminthic infections of medical interest. The portal of entry of microfilariae to the pericardial space is still a speculation. It might have lodged itself through blood stream subsequent to development of pericarditis. As microfilariae are capable of penetrating the tissues of the vector, they can freely move in and out of small, delicate blood, and lymphatic capillaries and tissues of the vertebrate host. [6] Also, filarial worms are highly immunogenic, eliciting a variety of cellular and humoral immune responses, leading to vasculitis incited by the filarial antigen. [7] Peripheral blood smears may be negative for Mf in cases of secondary manifestations of filariasis. [3],[4],[8] In this case also peripheral blood smears were negative. Clinical picture did not give any clue. Tuberculosis and viral etiology were ruled out. Radiological and electrocardiographic evidence of pericardial effusion and demonstration of Mf in the pericardial fluid and therapeutic response to DEC established the diagnosis of filarial pericardial effusion. Although microfilariae in unusual sites are considered incidental findings, the association of microfilariae with debilitating conditions suggests that it may be an opportunistic infection or it may be coincidental with various neoplasms. On the basis of existing evidences we suggest that some of the cases labeled as unresolving pericarditis, especially those from endemic areas, might be of filarial origin. It is therefore emphasized that a thorough examination of the aspirated fluid for Mf is warranted in all patients with unexplained pericardial effusion. [9] Wet mount examination of centrifuged fluid deposits has an established role in Clinical Microbiology in diagnosing clinically unsuspected cases. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10021f1.jpg] [mb10021f2.jpg] |
| |||||||||

{kind=link}
{kind=link}