 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
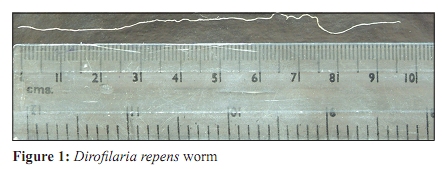
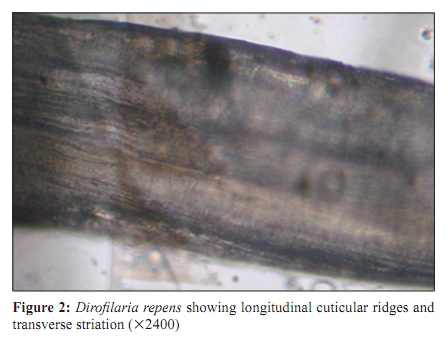
Indian Journal of Medical Microbiology, Vol. 28, No. 1, January-March, 2010, pp. 75-77 Case Report Dirofilariasis: A rare case report *R Singh, JV Shwetha, JC Samantaray, G Bando Department of Microbiology (RS, JVS, JCS), AIIMS, Ansari Nagar, New Delhi - 110 029, Ministry of Defence (GB), Ordnance Factory Hospital, Badmal, Bolangir, Orissa - 767 770, India Correspondence Address:Department of Microbiology, AIIMS, Ansari Nagar, New Delhi - 110 029, India, drrakesh1976@yahoo.com Date of Submission: 28-Mar-2009 Code Number: mb10022 PMID: 20061774 DOI: 10.4103/0255-0857.58739 Abstract Human dirofilariasis is a zoonotic infection most commonly caused by Dirofilaria repens. It has not been widely recognized in India. There is probably a focus of human infection with D. repens in Kerala. We report the first case of dirofilariasis, from the Eastern-part of India, to the best of our knowledge. Among the documented cases of human dirofilariasis caused by D. repens, recorded in India, most of them had ocular infections and few had subcutaneous involvement of the face. This is the first case report of human dirofilariasis from India involving the lower part of human body.Keywords: Dirofilariasis, Dirofilaria repens, Dirofilaria immitis Introduction The genus Dirofilaria includes various species that are natural parasites of dogs, cats, foxes and wild mammals. [1] Human infection caused by this genus is called dirofilariasis. It is a zoonotic infection and seen world-wide. It is caused by D. repens, D. immitis, D. tenuis, D. ursi etc. [2] D. repens is commonly encountered in the subcutaneous tissues of dogs while D. immitis in the right ventricle and pulmonary artery of the dogs. [1] Human dirofilariasis has not been widely recognized in India, but there is probably a focus of human infection with D. repens in Kerala. [1] The disease is relatively common in Sri Lanka, [3] which is geographically close to Southern India. Most of the documented cases of human dirofilariasis recorded in India presented with ocular infections. [4],[5],[6] First human case of pulmonary dirofilariasis in India, caused by D. immitis, was isolated from a child manifesting as portal cavernoma with pulmonary dirofilariasis detected at autopsy. [7] Culex, Aedes, Armigeres and Anopheles mosquitoes are vectors for this parasite, which take up the microfilaria (mf-L1) while feeding on an infected host. Microfilaria develops in the malpighian tubules to the infective third stage larva (L3) and then migrates to the proboscis through the body cavity. Transmission takes place when a potential vector bites dogs or other hosts including humans during a subsequent blood meal. [1] We report a scrotal, subcutaneous D. repens seen in a patient from Orissa. It is the first case to the best of our knowledge from Eastern India. All cases of subcutaneous dirofilariasis from India involved the face. [8],[9] This is the first case of subcutaneous dirofilariasis involving the lower part of human body. Case Report A 40-year-old male from the defence, and a resident of Orissa, presented with painful swelling in right upper-part of scrotal region for a period of five days. It was of the size of a peanut. One similar episode occurred in the right lower-part of scrotal region four years ago which resolved on conservative management. This time it didn't respond to antibiotics. There was no history of visit to Kerala, Karnataka and Sri Lanka. There was no history of exposure to dogs and cats. A worm was extracted and preserved in formalin. The preserved worm and the fluid aspirate from the scrotal cyst were sent to our laboratory for identification. Postoperative events were uneventful. Morphology The worm was thin, cylindrical, greyish and measured about 10.5 cm in length with a maximum diameter of 286 μm [Figure - 1]. The anterior end was rounded and of greater diameter than the posterior end. The cuticle of the worm was thick and had marked longitudinal ridges with transverse striations as shown in [Figure - 2]. Based on the size and cuticular morphologic features, the worm was identified as a female D. repens. The fluid aspirate did not contain any microfilaria. Discussion Cases of human dirofilariasis caused by Dirofilaria repens, have been reported widely throughout Asia, Europe and Africa. Reports of this infection from India are however limited. [4] The first reported case of human ocular dirofilariasis in India occurred in Kerala in 1976, June, [10] and the first reported case of subcutaneous dirofilariasis caused by D. repens was in June 2004 from the same region. [8] Kerala is considered an endemic for dirofilariasis. [1] While it is considered endemic in southern India, there are few case reports from the Northern [5] or Western parts [7] of India. This is the first case from the Eastern part of India to the best of our knowledge. Most of the documented cases of human dirofilariasis recorded in India had ocular infections, although there are a few case reports of subcutaneous dirofilariasis. All these cases involved the face. [8],[9] The present case is the first report of subcutaneous dirofilariasis involving the lower part of the human body from India. Genital area is the most common site for subcutaneous dirofilariasis in Sri Lanka [3] and this is thought to reflect the biting patterns of the mosquito vector. [11] D. repens[1] is the most common causative agent while in a few cases D. immitis[7] is also recorded as a causative agent of dirofilariasis from India. Most parasitologists believe that D. tenuis is restricted to the U.S.A. [8] However, D. tenuis infection is also reported from India. [12] D. repens is identified by the presence of external longitudinal cuticular ridges and transverse striation, there are other Dirofilaria, which shows these morphology. Exact identification of species may be possible only after studying the fully matured worm. However, D. immitis can be differentiated from D. repens by the absence of longitudinal ridges and transverse striation. [8],[9] Human Pulmonary Dirofilariasis (HPD) is mostly caused by D. immitis. [11] Patient may present with coin lesion in the chest X-ray, which were always diagnosed erroneously as malignant neoplasiae. [2],[11] Subcutaneous dirofilariasis is mostly caused by D. repens in Asia. [8] Patients usually present with single migratory nodules which may or may not be tender. [8] In our case the patient harboured the worm for probably more than four years. It was in the lower-part of the scrotal region and then migrated to the upper-part of scrotal region. Single worm has been isolated from the nodule in all the cases of subcutaneous dirofilariasis. [1],[8] Surgical removal of the worm is the treatment of choice. There is no need for chemotherapy as microfilaraemia is extremely rare. [1],[8] Human cases of dirofilariasis are most probably underreported because many of them remain undiagnosed or unpublished. [9] Dirofilariasis should be considered a differential diagnosis for single migratory subcutaneous swellings. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10022f2.jpg] [mb10022f1.jpg] |
| |||||||||

{kind=link}
{kind=link}