 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 100-106 Review Article Prevention and control of health care-associated infections through improved hand hygiene E Mathai, B Allegranzi, C Kilpatrick, *D Pittet World Health Organization Patient Safety (EM, BA, CK, DP), World Health Organization, Avenue Appia, 1211 Geneva 27, Switzerland, Infection Control Programme (DP), University of Geneva Hospitals and Faculty of Medicine, 4 Rue Gabrielle Perret-Gentil, Geneva, Switzerland Correspondence Address: *World Health Organization Patient Safety, World Health Organization, Avenue Appia, 1211 Geneva 27, Switzerland, Didier.Pittet@hcuge.ch Date of Submission: 15-Feb-2010 Code Number: mb10033 PMID: 20404452 DOI: 10.4103/0255-0857.62483 Abstract Determined actions are required to address the burden due to health care-associated infections worldwide and improve patient safety. Improving hand hygiene among health care workers is an essential intervention to achieve these goals. The World Health Organization (WHO) First Global Patient Safety Challenge, Clean Care is Safer Care, pledged to tackle the problem of health care-associated infection at its launch in 2005 and has elaborated a comprehensive set of guidelines for use in both developed and developing countries worldwide. The final version of the WHO Guidelines on Hand Hygiene in Health Care was issued in March 2009 and includes recommendations on indications, techniques, and products for hand hygiene. In this review, we discuss the role of hands in the transmission of health care-associated infection, the benefits of improved compliance with hand hygiene, and the recommendations, implementation strategies and tools recommended by WHO. We also stress the need for action to increase the pace with which these recommendations are implemented in facilities across India.Keywords: Alcohol-based hand rubs, guidelines, hand hygiene, health care-associated infection, international health, intervention, prevention and control of infection Introduction Estimates indicate that hundreds of millions of patients suffer from health care-associated infections (HCAI) each year worldwide. [1] The most common HCAI are urinary tract, surgical site, lower respiratory tract and bloodstream infections. In addition to increased morbidity and mortality, these infections contribute significantly to the financial burden borne by patients, their families, and the health care system. The increasing incidence of HCAI with antimicrobial-resistant bacteria further complicates the issue. Although the risk of acquiring these infections exists worldwide, the risk and impact are likely to be higher in resource-constrained settings where compliance with standard recommendations for infection prevention and control is generally not optimal. The capacity of existing systems to respond to the increased demand associated with HCAI, such as length of stay, cost, effective antimicrobial therapy and advanced technology is also limited in such settings. A large proportion of HCAI is preventable. In October 2004, heads of governmental agencies, policy-makers, and patient groups came together for the first time from all corners of the globe to advance the patient safety goal of "First, do no harm" and reduce the adverse health and social consequences of unsafe health care. The World Health Organization (WHO) contributes to this effort through the Patient Safety Programme with its First Global Patient Safety Challenge "Clean Care is Safer Care" (CCiSC), launched in 2005 and dedicated to the prevention of HCAI. One of the important recommendations for reducing HCAI is compliance with hand hygiene practices. Although maintaining hand hygiene is a simple act that should be routine behaviour among health care workers (HCWs), data from studies worldwide show that compliance is universally low. [1],[2] To achieve sustained improvement in hand hygiene, determined efforts are required at the point of care. For this reason, the core focus of CCiSC is on improving hand hygiene in health care and one of its main outputs, the WHO Guidelines on Hand Hygiene in Health Care, [1] (available at: http://whqlibdoc.who.int/publications/2009/9789241597906_eng.pdf; accessed 6 November 2009) provides detailed recommendations and tools (available at: http://www.who.int/gpsc/5may/tools/en/index.html; accessed 6 November 2009) to facilitate change. This review considers the role of hands in transmission of HCAI and examines the recommendations and methods for improving compliance with hand hygiene during routine patient care activities in health-care facilities. It also highlights some of the tools developed by CCiSC to achieve improved compliance. Aspects of surgical hand preparation are not addressed. Hands and HCAI Many studies confirm that pathogens implicated in HCAI can be isolated from the normal intact skin of upper extremities, including hands. [3],[4],[5] The resident flora of the skin consist mostly of bacteria that reside long-term under the superficial cells of the stratum corneum and on the surface of the skin. Staphylococcus epidermidis is the predominant species and oxacillin resistance is very high, especially among those carried by HCWs. [1],[3] Transient flora include bacteria, viruses and fungi on the skin surfaces that are acquired through direct skin contact or contact with contaminated environmental surfaces. These can be recovered from the skin only for short periods of time and do not usually multiply on skin surfaces. However, they can become temporarily resident and also multiply. [1],[3] Microorganisms that are part of the transient flora are most commonly associated with HCAI and are readily removed during routine hand hygiene procedures. [1],[3] The rate of hand contamination among HCWs varies. S. aureus, including methicillin-resistant S. aureus (MRSA), is among the most frequent causes of HCAI and often colonizes hands. Different studies show hand contamination rates of 10-78% among HCWs with S. aureus. [3] Similarly, very high rates of contamination are documented for other Gram-positive bacteria such as vancomycin-resistant enterococci (VRE) and Clostridium difficile, as well as several well-known HCAI causing Gram-negative bacilli. Depending on the species, the duration for which these can persist varies and can be for several hours on the skin, and even for weeks and months on environmental surfaces. [3] Five sequential steps can be considered important in the transmission of nosocomial pathogens from one patient to another through HCWs' hands: [1],[6]
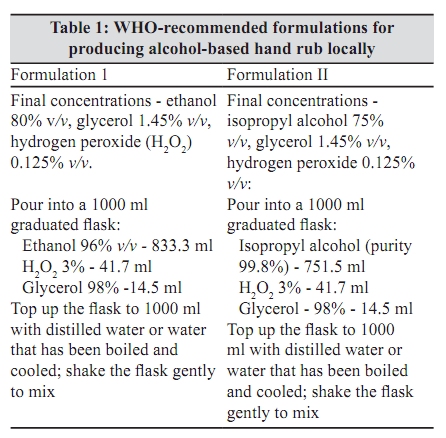
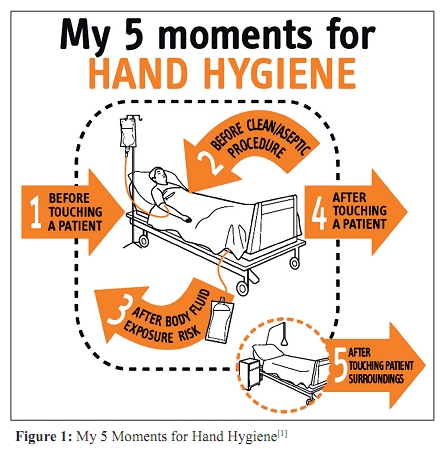
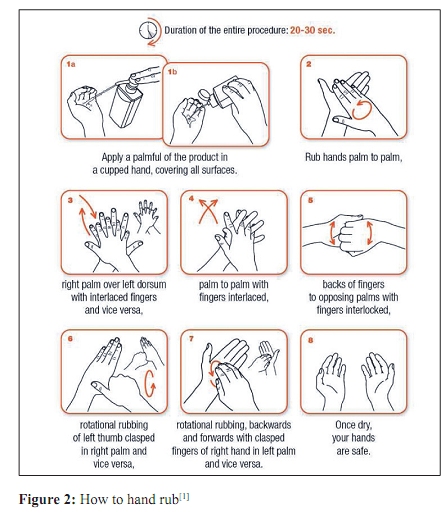
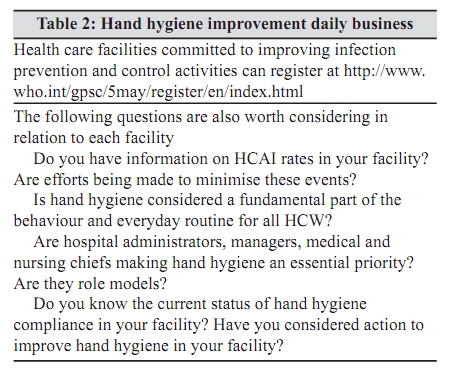
Preventing Transmission of Nosocomial Pathogens Through Hands The link between hand hygiene and the prevention of the spread of disease has been established only in the last 200 years. As early as 1847, Ignaz Semmelweis in Vienna, Austria, documented evidence to demonstrate the effect of hand hygiene in preventing nosocomial infections. [1] Semmelweis was a house officer at one of the two obstetric clinics at the Vienna General Hospital and observed that maternal mortality rates were much higher in the clinic where doctors delivered the women than in the one where midwives were in charge of births. He also noted that doctors and medical students often came directly to the labour room after having performed autopsies and retained a disagreeable odour on their hands, despite hand washing with soap and water. He hypothesised that "cadaverous particles" were transmitted by the hands of doctors and students, thus causing puerperal fever, and he recommended hand antisepsis with chlorinated lime solution, particularly after leaving the autopsy room. Following the implementation of this measure, the mortality rate dropped dramatically in the clinic most affected. Studies during the past few decades clearly show that a variety of hand hygiene methods reduce bacterial load significantly and prevent cross-transmission and HCAI. [1],[6],[20] An early prospective controlled trial [21] demonstrated that infants cared for by nurses who did not wash their hands after handling an index infant colonized with S. aureus acquired the organism significantly more often and more rapidly than those cared for by nurses who used hexachlorophene to clean their hands between infant contacts, thus providing compelling evidence for efforts to improve hand hygiene. Other studies have confirmed this finding in a variety of health care settings. [1],[22],[23],[24],[25] There is also good evidence to show that hand hygiene reduces the risk of transmission of infections in the community. [26],[27],[28] A few studies do not show a direct correlation between improved hand hygiene and reduction in HCAI. [29] Reduction in HCAI without a significant increase in hand hygiene compliance is also documented. [30] Some of these findings are related to differences in measurements, [2] given that there was no universally accepted method of measuring compliance or HCAI until recently. [1] This greatly affected comparability of data. Most studies neither address the quality of products used for hand hygiene nor compliance with recommended procedures for performing hand hygiene, but simply observe whether hand hygiene was performed for certain indications. There are also differences in the indications for hand hygiene in different studies. [1] Another factor to be considered while evaluating reports is that hand hygiene may not be implemented as a single intervention to reduce HCAI. In this scenario, models using available data demonstrate that interventions aimed at hand hygiene improvement can significantly contribute to reducing HCAI. [31],[32] Most guidelines for infection prevention and control include appropriate hand hygiene as a key recommendation. The methods used for hand hygiene during routine patient care include hand washing with plain or antimicrobial soap (the latter referred to as hygienic hand wash) and hand rubbing with alcohol-based or other antiseptic-based hand rubs. [1] Different terms such as hand disinfection, hand antisepsis, hygienic hand antisepsis, or hygienic hand rubbing, among others, are used in the literature to name these procedures. The recommendations in the WHO Guidelines on Hand Hygiene in Health Care are as follows: [1] "wash hands with soap and water when visibly dirty or visibly soiled with blood or other body fluids or after using the toilet; if exposure to potential spore-forming pathogens is strongly suspected or proven, including outbreaks of Clostridium difficile, hand washing with soap and water is the preferred means; use an alcohol-based hand rub as the preferred means for routine hand antisepsis if hands are not visibly soiled; if alcohol-based hand rub is not obtainable, wash hands with soap and water". Products for Hand Hygiene With the exception of non-medicated soap, every new formulation for hand antisepsis, should be tested to demonstrate that it has superior antimicrobial efficacy over plain soap or meets an agreed performance standard. [1],[33] In Europe, the most commonly used methods are those of the European Committee for Standardisation (Comité Européen de Normalisation, CEN). In the USA and Canada, these formulations are regulated by the Food and Drug Administration (FDA) and Health Canada, respectively, which refer to the standards of ASTM International, originally known as the American Society for Testing and Materials (ASTM). All these tests have limitations. Using a well-designed protocol that closely simulates the recommended field use of the formulation is most likely to yield useful data on its potential to interrupt transmission of pathogens by hands in healthcare settings. Hand hygiene has been performed traditionally by hand washing and is effective for the mechanical removal of extraneous matter. Plain soaps that are detergent-based have minimal microbicidal activity and may fail to fully remove pathogens from hands. [1],[34] Soaps may also be associated with skin irritation and dryness and can occasionally become contaminated with bacteria. [35],[36] Detergent formulations with additional antiseptics, such as chlorhexidine gluconate and triclosan (medicated soaps), are also widely available for hand washing with the former formulations being most common. These may be more effective than plain soap, but the activity depends on the chemical, concentrations used, duration of exposure, temperature, or the presence of organic matter. [1],[3] Most of these are relatively safe for use in hand hygiene products, but there is variability in the rapidity with which they act and in residual action. There are also growing concerns on resistance development and cross-resistance to antibiotics. [37] Alcohol-based formulations containing ethanol, isopropanol, n-propanol or a combination of these, are used for handrubbing. Alcohols have germicidal activity against vegetative bacteria, Mycobacterium tuberculosis, a variety of fungi, and several enveloped viruses, and are most effective at concentrations of 75-85%. [1],[3] However, they are ineffective against spores, protozoan cysts, and less effective against some viruses. Although there is evidence to show that alcohol has action against rotavirus, adenovirus, and polio virus, the activity depends on the alcohol, concentration, time of exposure, viral load and presence of proteinaceous materials. [3] A study using influenza A virus H1N1 showed alcohol-based handrubs and handwashing to be highly effective in eliminating the virus. [38] Compliance is much higher with alcohol-based hand rubs [39] and the risk of acquired resistance is insignificant. [3] The action of alcohol is rapid, but there is little residual activity. [3] For routine patient care, rapid action is critical, persisting action being significantly more important for surgical hand preparation. [33] Alcohols are not cleansing agents and, therefore, they are not recommended when hands are visibly soiled. Whether adding antiseptics such as chlorhexidine gluconate to alcohol has additional benefit in terms of clinical effectiveness remains to be further determined. [40],[41] Recent reports suggest than hand rubs other than alcohol can also be effective in eliminating microorganisms. [42] More data are required before conclusions can be drawn. Comparing different products available for hand hygiene is not easy for several reasons. These include the plethora of products available in different countries, variations in efficacy depending on test conditions, such as concentration, temperature, presence of organic matter, inherent problems associated with all current testing methods, and lack of universally-applied test methodologies. Although there is evidence that some medicated soaps have better activity as compared to plain soap, their superiority for routine hand hygiene has yet to be proved. Evidence is steadily accumulating to establish that alcohol-based hand rubbing is more effective in reducing bacterial load on hands, cross-transmission and HCAI, than hand washing with either plain or antimicrobial-containing soap. [1],[3],[43] However, as mentioned above, there are specific situations where hand washing is more effective and therefore recommended. While selecting a product, [1] one needs to consider efficacy, cost, aesthetic preferences, such as colour, texture, and fragrance, and practical issues such as availability, ease of dispensing, or preventing contamination. Skin tolerance by HCWs is a critical consideration since these products will have to be used multiple times each day and several formulations have the potential to cause skin irritation and allergy. For hand rubs, drying time is also an important factor that affects compliance. Although some reports suggest that alcohol-based rinses may be more effective than gels, [44] compliance should receive high consideration while choosing a product. WHO recommends two alcohol-based hand rub formulations that can be produced locally [Table - 1] . [1] Involving HCWs in the choice of the product and pilot testing for acceptability is recommended since it can increase compliance. Hand Hygiene: How and When? The purpose of hand hygiene is to prevent colonisation and infection in the patient, colonisation and infection in the HCW, and contamination of the environment. Therefore, an opportunity for hand hygiene arises every time that there is a possibility of microorganism transfer from one skin or inanimate surface to another surface. [6] To facilitate easy identification of opportunities for hand hygiene by HCWs and to meet the needs for training, compliance measurements, and comparable performance reporting, CCiSC recommends a "five moments" approach. [45] This is a simple concept which encompasses the different activities in the complex sequence of care and can be summarized as follows: 1) Before touching a patient; 2) Before a clean/aseptic procedure; 3) After body fluid exposure risk; 4) After touching a patient; and 5) After touching patient surroundings [Figure - 1]. The detailed recommendations can be found in the WHO Guidelines on Hand Hygiene in Health Care as well as in the original publication. [45] Adherence to recommended techniques, such as the volume of product to be used, hand surfaces to clean, and duration for hand washing and hand rubbing, are important for effectiveness. [1] [Figure - 2] illustrates the recommended technique for hand rubbing using an alcohol-based formulation that requires 20 to 30 seconds. Hand washing with soap and water requires additional steps (rinsing and drying) and usually takes between 40 and 60 to 90 seconds for completion. Because wet hands can readily acquire and spread microorganisms, proper drying of hands [46] and single-use towels are necessary. Care must be taken to avoid recontamination of hands while drying and turning off the tap. Soap and alcohol-based rubs are not recommended for concomitant use. Implementation Strategies Improving hand hygiene depends on system and behavioural changes. Taking into account interventions required for a change in behaviour, CCiSC recommends a multimodal strategy and has developed a Guide to Implementation and a range of tools to facilitate (available at: http://www.who.int/gpsc/5may/tools/en/index.html; none accessed 6 November 2009) improvement in hand hygiene in health care facilities worldwide. The five essential elements of the strategy are: a) system change, including availability of alcohol-based hand rub at the point of patient care and access to a continuous safe water supply, soap and towels; b) training and education of HCWs; c) monitoring of hand hygiene practices and performance feedback; d) reminders in the workplace; and e) the creation of a safety culture with the participation of both individual HCWs and senior hospital managers. Five sequential steps are recommended for implementation of these strategies. (Available at: http://www.who.int/gpsc/5may/Guide_to_Implementation.pdf;none ; accessed 6 November 2009). These are facility preparedness - readiness for action; baseline evaluation - establishing the current situation regarding hand hygiene compliance; implementation - introducing the improvement activities; follow-up evaluation - evaluating the implementation impact; and an action planning and review cycle - developing a plan for a minimum of the following five years. These recommendations can be modified and adapted to suit requirements and resources at each facility. Measuring compliance with hand hygiene is essential to understand the current situation, to facilitate change, and to measure the impact of interventions. [2] There are different methods recommended and these include direct observation, automated monitoring systems, product consumption, and self reporting by HCWs. Monitoring HCAI rates is necessary to understand the impact of hand hygiene improvement. Uniformity in the methods used for these measurements is essential for comparability. The method recommended by WHO for measuring compliance (Sax H, Allegranzi B, Chraiti M-N, Boyce J, Larson E, Pittet D. The World Health Organization hand hygiene observation method. Am J Infect Control 2009; 37:827-34: now published) and the related tools can be obtained from the web site. Available at: : http://www.who.int/gpsc/5may/tools/evaluation_feedback/en/index.htmlnone . Accessed 6 November 2009. Need for Action HCAI rates remain high despite an increase in awareness and actions to reduce these infections, partially due to increasingly complex health care interventions. The momentum created by CCiSC is significant and reports from around the world show an upward trend in compliance with hand hygiene. [Allegranzi B, Sax H, Bengaly L, Richet H, Minta DK, Chraiti M-N, et al. Successful implementation of the WHO hand hygiene improvement strategy in a referral hospital in Mali, Africa. Infect Control Hosp Epidemiol 2010; 31:133-41. - now published] Health care facilities in different parts of the world have already adopted hand hygiene as an essential intervention for reducing HCAI. Several countries have initiated nationally coordinated activities (available at: http://www.who.int/gpsc/national_campaigns/en/; none accessed 6 November 2009) to promote hand hygiene in health care, but the question of sustainability remains. Although coordinated efforts exist in India to promote hand hygiene in communities and schools to reduce the burden of diarrhoea and other infections, there is a paucity of information on activities to promote hand hygiene in health-care facilities. There is also a lack of satisfactory information from India on HCAI in general. Sporadic reports document the role of hands in spreading infection and isolated efforts at improving hand hygiene across the country. [47],[48],[49],[50] It is necessary to increase the pace of activities to reduce HCAI and to effectively engage millions of HCWs in different types of health-care facilities in this effort. The Director General of Health Services of India confirmed his resolve to promote activities at a national level to reduce HCAI by signing a commitment with CCiSC on July 14 2006. (Available at: http://www.who.int/patientsafety/events/06/statements/India_pledge.pdf.none Accessed 6 November 2009). "Developing or enhancing ongoing campaigns at national or sub-national levels to promote and improve hand hygiene among health care providers" is among the activities committed to through this pledge. Professional societies have an important role to play in bringing this commitment into practice through advocacy and contributions to the required technical expertise. Conclusion Although considerable progress is being made in health care facilities worldwide to reduce HCAI by adherence to hand hygiene recommendations, the need to further scale up and ensure that it becomes an essential element of quality of care is evident. Lack of comparable and good quality data is one concern to be addressed. There are also several questions to be answered, especially in areas related to interventions, implementation strategies in different parts of the world, and measurements to evaluate impact. National, facility and individual level commitment, co-operation, and actions are required to address these deficiencies and to make sustainable improvements. Promoting the application of the "5 moments" at the point of care [Figure - 1] is one simple step that each HCW and health-care facility can act on now [Table - 2]. Acknowledgments The authors thank all members of the Infection Control Programme, University of Geneva Hospitals, and team members of the WHO First Global Patient Safety Challenge "Clean Care is Safer Care", and Rosemary Sudan for expert editorial assistance. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10033f1.jpg] [mb10033t2.jpg] [mb10033t1.jpg] [mb10033f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}