 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
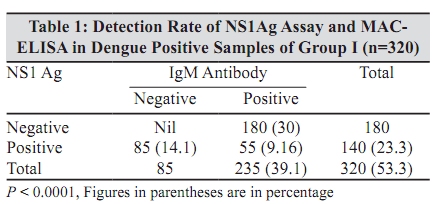
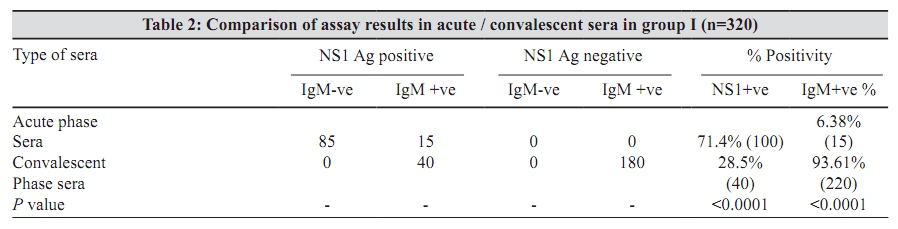
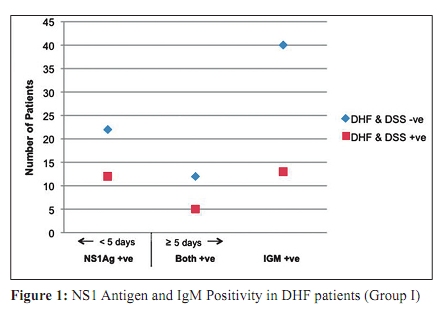
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 107-110 Original Article Dengue NS1 antigen detection: A useful tool in early diagnosis of dengue virus infection S Datta, *C Wattal Department of Clinical Microbiology, Sir Ganga Ram Hospital, Rajinder Nagar, New Delhi - 110 060, India Date of Submission: 23-Jun-2009 Code Number: mb10034 PMID: 20404453 DOI: 10.4103/0255-0857.62484 Abstract Purpose: This study was undertaken to evaluate the efficacy of NS1 antigen (Ag) assay as an early marker for dengue virus (DV) infection.Materials and Methods: Group I evaluated the performance of NS1 antigen (Ag) assay in comparison to MAC-ELISA and their detection rate when performed together in a single sample. Six hundred acute/early convalescent sera were screened by both the assays. Group II evaluated the efficacy of a single assay in 30 acute phase sera of paediatric OPD patients screened only by NS1 Ag assay. Group III evaluated the specificity of NS1 assay in comparison to MAC-ELISA on 40 samples included as controls. Results: In Group I, 140 (23.3%) and 235 (39.1%) samples were positive by NS1 assay and MAC-ELISA respectively. The detection rate increased to 320 (53.3%) when both the assays were used together on a single sample. NS1 Ag positivity varied from 71.42% to 28.4% in acute and early convalescent sera, conversely IgM detection rate was 93.61% and 6.38% in early convalescent and acute phase sera respectively (P < 0.0001). In Group II, 66.66% (20) samples were positive by NS1 assay. All the samples in Group III were negative showing 100% specificity of both the assays. Conclusion: NS1 Ag assay holds promise in early diagnosis of dengue infection. When used in combination with MAC-ELISA on a single sample it significantly improves the diagnostic algorithm without the requirement of paired sera. Keywords: Acute phase sera, dengue, laboratory diagnosis, MAC-ELISA, NS1 antigen assay Introduction Dengue fever is an acute febrile arbo-viral disease affecting the tropical and subtropical regions of the world. The incidence of this disease has increased over the last 50 years with 2.5 billion people living in areas where dengue is endemic. [1] It affects up to 100 million people each year, with 500,000 cases of dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) and around 30,000 deaths, mostly amongst children. [2] In view of the high mortality rate and to reduce the disease burden, it is imperative to have a rapid and sensitive laboratory assay for early detection of the disease. The major diagnostic methods currently available are viral culture, viral RNA detection by reverse transcriptase PCR (RT-PCR) and serological tests such as an immunoglobulin M (IgM) capture enzyme-linked immunosorbent assay (MAC-ELISA). However, early dengue diagnosis still remains a problem, as all these assays have their own pitfalls. The first two assays have restricted scope as a routine diagnostic procedure. Viral isolation by cell culture and subsequent detection by immunofluorescence, though the gold standard, [3] cannot be used as a routine diagnostic procedure due to its low sensitivity, laborious procedure and time consumption. [4],[5] The requirement of a highly trained staff, the need of a sophisticated equipment as well as the cost factor associated with molecular methods has limited its application as a routine diagnostic assay. The MAC-ELISA, which is a commonly used assay, has a low sensitivity in the first four days of illness. [6] The requirement of paired sera at acute and convalescent phase, which improves the accuracy of the diagnosis, further delays it. NS1 (non-structural protein 1) is a highly conserved glycoprotein that is essential for the viability of DV and is produced both in membrane-associated and secretory forms by the virus. [7] Enzyme-linked immunosorbent assays (ELISA) directed against NS1 antigen (NS1 Ag) have demonstrated its presence at high concentrations in the sera of DV infected patients during the early clinical phase of the disease. [7] The detection of secretory NS1 protein represents a new approach to the diagnosis of acute DV infection. In this study, an attempt has been made to evaluate the NS1 Ag assay as a new diagnostic tool for early diagnosis of dengue virus infection in a tertiary care hospital. Material and Methods Patients and Study-design: Six hundred and seventy blood samples were screened from clinically suspected cases of dengue fever reporting at our centre from January - December 2008. The demographic profile was taken from HIS (hospital information system). Mean age of the study population was 20 years (range seven months - 49 years) and the sex ratio (male/female) 1.2. The serum samples comprised of both acute and early convalescent phases depending on the reporting time of the patients. Acute phase serum samples were collected from patients who reported within one to four days of fever and early convalescent phase serum were collected from patients who came with history of fever for > 5 days. The samples were divided into three study groups. Group I comprised of 600 samples obtained from 600 patients of suspected cases of dengue fever classified as undifferentiated fever/dengue fever (DF) / DHF (WHO classification). All adult samples both from out patients department (OPD) and in-patients department (IPD) and only paediatric IPD patients were included in this group. Single blood sample drawn from the patients were screened by both NS1 Ag assay and MAC-ELISA. Group 1 evaluated the performance of NS1 Ag assay in comparison to MAC-ELISA in acute or early convalescent sera and the detection rate when performed together in a single serum sample. The impact of NS1 Ag as an early marker of DHF was also evaluated. Group II comprised of 30 samples from paediatric OPD patients classified as undifferentiated fever or DF (WHO classification). All presented within first four days of fever. Acute phase sera drawn from the study group was screened only by NS1 Ag assay. This group evaluated the diagnostic efficacy of a single assay in acute phase sera to confirm its use as a cost effective test of choice in the first four days of infection. Since this group was a compliant group and attended the OPD at regular intervals, paired samples of patients who were negative by NS1 Ag assay in acute phase were subsequently screened for antibodies in the early convalescent phase. Group III was the control group with 40 samples. Twenty samples were from patients with fever due to a proven aetiology other than dengue [enteric fever (13), bacterial meningitis (2), UTI (5)] and twenty samples were obtained from healthy blood donors. All the 40 samples were screened by both the assays. Seroassays NS1 Ag assay: The test was performed using new PLATELIA TM Dengue NS1 Ag assay (BIORAD, Marnes-la-coquette, France). This is a single-step sandwich-format micro plate enzyme immunoassay to detect dengue virus NS1 Ag in human serum or plasma. Murine monoclonal antibodies are used to capture and detect NS1 antigen. Sample results were expressed in terms of index value. According to the manufacturer's recommendations, samples were considered (i) nonreactive for dengue virus NS1 Ag if index value < 0.5, (ii) equivocal for dengue virus NS1 Ag if between 0.5 to 1.0, and (iii) reactive for dengue virus NS1 Ag if index value 1.0 or more was obtained. The Dengue IgM Capture ELISA or MAC ELISA (PANBIO diagnostics, Brisbane, Australia) was used to detect the presence of dengue specific IgM antibodies in the patient's sera. Sample results were expressed in terms of PANBIO units as per the recommendations of the manufacturer. Samples were considered (i) non-reactive for dengue IgM antibody if < 9 PANBIO units (ii) equivocal in range of 9-11 (iii) reactive for a value of> 11 PANBIO units. Statistical analysis The Fisher's exact test was used to find out the P values of the results. P value < 0.05 was considered significant. 95% confidence interval [CI 95 ] was calculated to get the interval of a particular patient-population parameter to indicate the statistical significance of the estimate. Results In Group I , of the 600 samples, 320 (53.33%) were positive either for NS1 Ag or IgM antibody or both [Table - 1]. A total of 140 (23.3%) samples were positive for NS1 Ag and 235 (39.1%) were positive for IgM antibody including those that were positive by both [Table - 1]. Both the assays, performed together on a single serum sample, significantly increased the detection rate to 53.3% (P < 0.0001). Of the total 140 NS1Ag positive samples, 71.42% (100) were from acute phase serum samples and 28.4% (40) were from early convalescent phase [Table - 2]. The NS1 Ag detection rate decreased from 71.42% in acute phase sera to 28.4% in early convalescent sera (P < 0.0001). All the 85 samples that were positive for NS1 Ag alone in this study group I belonged to acute phase sera [Table - 2]. Conversely, of the 235 IgM positive samples, 93.61% (220) were from early convalescent phase and only 6.38% (15) were positive from acute phase sera. All the 180 samples that were only IgM positive belonged to early convalescent phase [Table - 2]. The seroposivity of IgM increased from 6.38% in acute phase sera to 93.61% in convalescent sera (P < 0.0001). Of the total 320 positive cases, 104 samples were from cases clinically suspected as DHF. All had a platelet count of ≤100,000 /µl (WHO cut off for platelet count for DHF). Seventy-four of the 104 clinically suspected DHF cases had no manifestations of DSS [Figure - 1]. They were all monitored closely following admission. Of these 74 cases, 34 (46%) [CI 95 ] 34.6-57.3%) were detected positive by NS1 Ag assay and 22 (29.7% [CI 95 ] 19.32%- 40.14%) of them were detected in the first four days of fever and were IgM negative. Thirty of these 104 cases were diagnosed as DSS. Seventeen (56.67% [CI 95 ] 38.94 -74.4%) were NS1 Ag positive and 12 (40% [CI 95 ] 22.47%-57.53%)) were detected in the first four days of fever and were IgM negative [Figure - 1]. However, 280 samples were negative by both the assays. All the thirty samples from study Group II were screened only for NS1 Ag and 20 (66.66%) were positive. All these 20 patients were classified as DF. All had normal platelet count (150000-450000/µl). The 10 NS1 Ag negative samples from patients with undifferentiated fever remained seronegative on subsequent screening at early convalescent stage. All the 40 samples from Group III were negative by both the assays. Discussion The results obtained were analyzed and evaluated. The role of NS1 Ag for early detection of DV infection is currently being evaluated by many investigators, without the requirement of paired sera. [4],[8] NS1 Ag circulates uniformly in all serotypes of dengue virus and it circulates at high level during the first few days of illness. [9] NS1 Ag levels varies from 0.04 - 2 µg/ml in acute-phase serum samples, to only 0 .04µg/ml or even less in convalescent phase serum. [6] This is the reason for its higher detection rate in acute phase sera. In our study, NS1 Ag positivity was 71.42% in acute phase sera in study group I. IgM positivity in the acute phase sera in this group was only 6.38%. Detection of specific IgM by MAC-ELISA is still used as the diagnostic technique for acute infection; its disadvantage being delayed appearance of antibodies from 5-10 days after the onset of illness in case of primary dengue virus infection and 4-5 days after the onset of illness in secondary infections. [7] The requirement of paired sera, subsequently in convalescent phase, if negative in acute phase also delays diagnosis. Our study demonstrated an IgM positivity of 93.61% in the early convalescent sera. Conversely, NS1 Ag positivity in early convalescent phase was 28.57%. The detection rate of IgM increased from 6.38% in acute phase sera to 93.61% in convalescent sera and NS1 Ag detection decreased from 71.4% in acute phase sera to 28.57% in early convalescent sera, which were both statistically significant. Similar findings were seen in other studies along with an increase in sensitivity of detection when both the assays were used together in a single sample. [10],[11] A statistically significant increase in detection rate was observed when both the assays were performed together in a single sample. The morbidity and the mortality of DHF can be reduced by early diagnosis, hospitalization and symptomatic care. In our study, 29.7% (22) of patients with DHF without DSS, and 40% (12) of patients with DSS were detected in the first four days of illness by NS1 Ag assay and they were all IgM negative [Figure - 1]. Thus NS1 assay expedited the laboratory confirmation within the first four days of illness. Studies claim that in addition to an early diagnosis, NS1 antigen may be an indicator of disease severity. [9] Libraty et al. observed that a very high concentration of NS1 antigen within 72 hours of illness identified patients at risk of developing DHF [12] though a quantitative estimation of NS1 Ag was not carried out in this study to confirm this observation. In group II, 66.66% were NS1 Ag positive. All the positive patients were classified as DF and they were all detected by NS1 Ag assay within the first four days of fever. Their platelet count remained normal throughout the illness. The assay could diagnose 66.6% cases of DF in the first four days of illness. The sensitivity of this assay was good, especially in samples collected from cases classified as DF. Samples from cases that were negative by NS1 Ag assay presented as undifferentiated fever and were subsequently screened for antibodies after five days of fever. All tested negative confirming the high specificity of this assay. The specificity of NS1Ag assay was also assessed from the control group which was 100%. In conclusion, this study substantiates that in comparison to MAC-ELISA, NS1 Ag assay is an effective tool for diagnosis of DV infection, especially within the first four days of illness. Early detection of DHF by NS1 assay can help in early confirmation and management of this vulnerable group. NS1 Ag assay, if used in combination with MAC-ELISA on a single serum sample of a suspected case, has the ability to improve the diagnostic algorithm contributing significantly to the clinical treatment and control of dengue viral infections. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10034t2.jpg] [mb10034f1.jpg] [mb10034t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}