 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
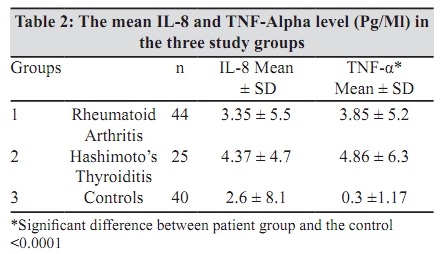
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 120-123 Original Article Immune responses to Epstein-Barr virus in individuals with systemic and organ specific autoimmune disorders *R Kannangai, J Sachithanandham, AJ Kandathil, DL Ebenezer, D Danda, Z Vasuki, N Thomas, SK Vasan, G Sridharan Departments of Clinical Virology (RK, JS, AJK, DLE, GS), Rheumatology (DD, ZV) and Endocrinology (NT, SKV), Christian Medical College, Vellore - 632 004, India Correspondence Address: Department of Clinical Virology, Christian Medical College, Vellore - 632 004, India, rajeshkannangai@hotmail.com Date of Submission: 02-Jul-2009 Code Number: mb10037 PMID: 20404456 DOI: 10.4103/0255-0857.62487 Abstract Purpose: Autoimmune diseases usually manifest in genetically predisposed individuals following an environmental trigger. There are several viral infections including Epstein-Barr virus (EBV) implicated in the pathogenesis of autoimmune disorders. The aim of this study was to look at the antibody pattern to EBV proteins in the plasma of both systemic and organ specific autoimmune disorders, estimate pro-inflammatory plasma cytokines (IL-8 and TNF-α) among these autoimmune patients and compare the observations with those in normal healthy controls.Materials and Methods: Samples from 44 rheumatoid arthritis patients, 25 Hashimoto's thyroiditis patients, appropriately age and sex matched healthy controls were tested for EBV IgM antibodies by an immunoblot assay and two cytokines (IL-8 and TNF-α) by commercial assays. Results: Among the rheumatoid arthritis patients, 23 (52%) were positive for EBNA1 antibody, while 13 (52%) of the Hashimoto's thyroiditis patients and 12 (30%) of the healthy controls showed similar bands. The intensity of the bands was high in the autoimmune patients when compared to the bands seen in control samples. The difference in the EBNA1 reactivity between rheumatoid arthritis patients and controls were significant (P = 0.038). There was a significant difference in the IgM reactivity to VCAp19 protein between patients and controls (P = 0.011). Conclusion: Our study showed an increased EBV activation among the autoimmune patient groups compared to the normal healthy controls. Further studies are required to delineate the association between the aetiology of autoimmune disorders and EBV. Keywords: Autoimmune disorder, EBV, Hashimoto's thyroiditis, rheumatoid arthritis Introduction Autoimmune diseases usually occur following an environmental trigger in genetically predisposed individuals. [1] There are several viral infections implicated in the pathogenesis of autoimmune disorders. Epstein-Barr virus (EBV) is presumed to be one among these, which behaves similarly, and its role in triggering autoimmunity has been reported in several diseases. [2],[3],[4] In developing countries like India, most of the individuals get infected with EBV in early childhood, with more than 90% children infected by the age of six. [5] Following EBV infections intense immune response against many virus specific proteins has been detected. [6] However, these immune responses never completely eliminate the virus and may lead to chronic immune complex disease. The exact mechanism involving EBV in the causation of systemic and organ specific autoimmune disease is elusive. Viral infections can be triggers to initiate disease by antigen release or formation of altered antigens or causing molecular mimicry by secretion of chemokines or cytokines. In our current study we have focused on association of EBV with two specific autoimmune diseases - rheumatoid arthritis and Hashimoto's thyroiditis. In rheumatoid arthritis the rheumatoid factor induces signalling from B-lymphocytes, which in turn re-activate the B-lymphocytes and the latent EBV infection. [7] Cytokines have been strongly implicated in the pathophysiological and pathogenetic mechanisms associated with autoimmune disorders by both clinical and experimental studies. [8] There are reports of increased expression of cytokines like IL-8, TNF-α in certain autoimmune disorders.[9],[10] In vitro studies have shown that viruses such as EBV and human herpes virus (HHV-6) can induce the production and release of IL-8. [11],[12] It is reported that patients with rheumatoid arthritis have very high EBV load in peripheral blood lymphocytes than healthy controls. [13] Patterns of antibody (IgG) to certain EB viral proteins like viral capsid antigen (VCA) and nuclear antigen (EBNA) can predict autoimmune disorders like multiple sclerosis. [14] The aim of this study was to investigate the antibody pattern to EBV proteins in the plasma of both systemic and organ specific autoimmune disorders and estimate plasma cytokines (IL-8 and TNF-α) among these autoimmune patients compared to normal healthy controls to ascertain the association of EBV with these two common autoimmune disorders. Materials and Methods The study was carried out in the department of Clinical Virology, of a tertiary care centre, in south India in the period from 2005 to 2008 following the approval from the institutional review board. Samples from 44 systemic autoimmune patients, 40 age and sex matched healthy controls and 25 organ specific autoimmune patients were collected. The controls were age, sex matched with the systemic autoimmune patients and fewer in number with more than one patient in the same age group. The autoimmune conditions were diagnosed by the treating physicians. These individuals were not on any anti-inflammatory drugs at the time of sampling. All the systemic autoimmune patients were diagnosed as rheumatoid arthritis, while all the organ specific patients were diagnosed to have Hashimoto's thyroditis. Rheumatoid arthritis was diagnosed using the American College of Rheumatology (ARC) criteria, 1987. A diagnosis of Hashimoto's thyroiditis was made based on the presence of a lobular thyroid gland and the presence of anti-thyroid antimicrosomal antibodies being positive (Serodia-AMC, Fujirebio Inc, Tokyo, Japan) in a titer of ≥ or equal to 80 2 (1:6400). Subjects who were either euthyroid, hypothyroid or hyperthyroid were all included in the analysis. Six ml of whole blood were collected in EDTA tubes from these volunteers after an informed consent. Plasma separated and stored in aliquots at -70 0C for the immunoblot analysis, TNF-α and IL-8 estimation. The antibody pattern was analyzed by testing the samples with an EBV IgM immunoblot (EBV-profile 2 EUROLINE, Euroimmune, Denmark). This provides a qualitative in-vitro assay for human antibodies to five different EBV antigens: VCA gp125, VCA p19, EBNA-1, p22, and EA-D. The manufacture's instructions were followed while carrying out the assay. In brief pre-treated strips with block buffer were incubated at room temperature with 1:101 diluted plasma samples for 60 minutes on a rocking shaker followed by washing and addition of enzyme conjugate (alkaline phosphatase conjugated anti-human IgM). After 60 minutes of incubation at room temperature the strips were washed again followed by the addition of substrate (NBT/BCIP) and incubation for 20 minutes at room temperature. The reaction was stopped by washing the strips with the addition of distilled water. The membrane strips were dried and automated evaluations of these strips for the analysis of different bands and the intensities were examined with EUROLineScan system provided by the manufacturer. The reading was taken by keeping the strips on a flatbed scanner (HP psc 1350) which enables the EUROLineScan to recognizes the position of the strips, identify the bands and measure its intensity. The quantitative detection of TNF-α and IL-8 were done by human TNF-α ELISA version 4 (Bender MedSystems GmbH, Vienna, Austria) and human IL-8/NAP-1 ELISA (Bender MedSystems GmbH, Vienna, Austria) respectively. The instruction of the manufacturers was followed while carrying out the assay. Respective plates were pre-coated with monoclonal antibody against TNF-α and IL-8. All the samples were tested in duplicate and the mean value was taken for analysis. The standards provided with the kits were used, for TNF-α standards ranged from 0-500 pg/ml while for IL-8 it ranged from 0-1000 pg/ml. An automated microplate washer (Elx 50, Bio-Tek instruments, Vermont, USA) was used for washing while an automated microplate reader (µQuant, Bio-Tek instruments, Vermont, USA) was used for measuring the OD reading. A standard curve was generated with the KC4 software (version 2.7 Bio-Tek instruments, Vermont, USA) and the concentrations were estimated for TNF-α using a 4 parameter curv and IL-8 using a polynomial curve. The EBV DNA viral load estimation by a real time PCR in plasma samples was also carried out in a proportion of individuals. This included 10 each of rheumatoid arthritis and Hashimoto's thyroiditis patients and three of the healthy controls. The in-house EBV quantitation real time PCR assay was designed to amplify the BNT p143 region. The standards were prepared using in-house plasmids. Probes for the detection of EBV DNA were labelled with reporter dyes Cy5 and black hole quencher (BHQ) at the 5′ and 3′ end, respectively (Metabion, Martinsried, Germany, Operon Biotechnologies GmbH, Cologne, Germany). Amplification of EBV DNA was done using 10µl of DNA extracts was added to 25 µl mix containing 12.5µl of QuantiTect Multiplex PCR NoROX master mix (Hamburg, Germany) and 0.075 µl (7.5 picomoles) of EBV primers, 0.05 µl (5 picomoles) of EBV probe. The thermal cycling conditions used to amplify EBV DNA were as follows 95°C for 15 min, 95°C for 45 sec, and 60°C for 75 sec for 50 cycles. The EBV DNA was amplified and detected using real time PCR (Rotor gene RG-3000, Corbett Research, Sydney Australia). Statistical analysis The comparisons of proportion of individuals' positive for different antibodies in the three groups were compared by c2 test. The mean of the cytokine levels estimated in the three groups were compared by ANNOVA test. All statistical tests were done using EPI info ver 6.04c. Results Among the rheumatoid arthritis patients, 23 (52%) were positive for EBNA1 antibody while 13 (52%) of the Hashimoto's thyroiditis patients and 12 (30%) of the healthy controls showed similar bands. The intensity as graded by the EUROLineScan system (1+ to 3+) of the bands was high in the autoimmune patients when compared to the bands seen in control samples. The numbers of samples showed 2+ or more reactivity in autoimmune patients were 2, 11, 13, 3 and 2 for VCAgp125, VCAp19, EBNA1, P22 and EA-D respectively. Among the controls all positive samples except 1 each for VCAgp125 and p22 had intensity of 1+ only. The difference in frequency of EBNA1 positivity between the three groups just fell short of significance (P = 0.08). Similar results were observed between EBNA1 reactivity among Hashimoto's thyroiditis patients and controls (P = 0.08). However, the differences in the EBNA1 reactivity between rheumatoid arthritis patients and controls were significant (P = 0.038). There was a significant difference in the IgM reactivity to VCAp19 protein between patients and controls (P = 0.011). Antibody to p22 was positive in 8 rheumatoid arthritis patients and 9 controls while it was negative in all the Hashimoto's thyroiditis patients. The immune reactivity to different antigens among the three study groups is shown in [Table - 1]. The mean IL-8 levels were 3.35, 4.37 and 2.36 pg/ml in the rheumatoid arthritis, Hashimoto's thyroiditis and the healthy control groups respectively. The TNF-α level in the above three groups were 3.85, 4.86 and 0.3 pgm/ul respectively. The TNF-α level was significantly higher in the patient groups (P < 0.001) while there was no significant difference in the IL-8 level between patients and control groups. This data is shown in [Table - 2]. All the 23 samples were negative for EBV DNA. Among these 23 samples tested, nine of the rheumatoid arthritis, seven of Hashimoto's thyroiditis and one normal healthy control showed IgM antibody to EBNA-1 protein. Discussion Both environmental and genetic factors contribute to the development of many autoimmune diseases. The causative environmental factors are still unknown in many of these diseases. One of the mechanisms in such disease conditions may be an altered immune response to opportunistic viruses like EBV. [2],[3] Our study compared the immune response against EBV in autoimmune patients with that of healthy individuals and certain proinlammatory cytokine levels. EBV serology consists of various markers that help to differentiate EBV infection as acute, latent infection or reactivation of latent infection. An IgM immune response against VCA and EBV EA are clear indication of the presence of recent infection. However, the presence of EBNA1 antibody is significant among the autoimmune patients and indicates reactivation of EBV infection rather than a recent acute infection. In India the median age of serconversion to EBV indicating exposure is very low 2.5 years and EBV becomes latent in a large number of exposed and infected individuals. [4] Although these EBNA are the antigens synthesized prior to the other antigens like VCA and EA they are the ones which presented to immune system only in the later stages and hence the delayed response. A significantly higher number of autoimmune patients in our study group had immune responses against these proteins especially EBNA and VCA suggestive of reactivation of a latent EBV infection. It is shown that the EBV infection may contribute indirectly to the pathophysiology of autoimmune diseases by impairing immune control of EBV replication, which in turn leads to increased exposure to EBV antigens and hence the chronic inflammation. [15] The other reason for the significant increase in the EBV IgM reactivity may be that rheumatoid factor (RF) can induce signalling from B cells that activates other B-cells and in turn lead to the activation of persistent EBV. [7] It is also demonstrated by in vitro assays that the saliva from Sjogren's syndrome can also activate the B cells at the inflammatory site in the presence of TGâ1 via triggering of the mitogen-activated protein kinase (MAPK) signalling pathway.[16] Recently, one of the studies from Taiwan demonstrated an association of EBV infection with SLE by demonstrating higher sero-reactivity (IgA anti-EBV EBNA1 and IgG anti-EBV DNase) and higher copy numbers of EBV genome. [17] However in our study group none of the 23 tested volunteers showed DNA in plasma. It would be ideal to see the EBV load in peripheral blood lymphocytes of the autoimmune patients and healthy controls. It is also shown that the first lupus-specific auto antibodies arise from particular antibodies directed against EBNA-1 and that infection with EBV is an environmental risk factor for SLE [18] The sequence of events in this case scenario is normal immunity, generation of anti-EBNA-1 antibodies following EBV infection, binding of these antibodies to lupus-specific autoantigens (Sm or Ro), followed by the development of more complex autoimmune responses, and leads to clinical disease. [18] Similar mechanism may be involved in the development of Rheumatoid arthritis. Our study also showed a significantly higher frequency of EBNA-1 antibody and reactivity to EA among the Hashimoto's thyroiditis patients compared to the healthy controls. This is probably related to induction of anti T3 antibodies. There are studies which showed associations of Hashimoto's thyroiditis with several viral infections [19] It is shown that the higher IgG antibody titers against viral capsid antigen (VCA) and positivity of antibodies against EA were significantly higher among patients with autoimmune thyroiditis compared to control group. [20] Our results were consistent with previous literature published on EBV serology in thyroiditis. The increase in the TNF-α activity seen in our patient group may be related to the ongoing inflammatory reactions. Though the IL-8 level was high among the patient group again an indication of chronic inflammation it was not statistically significantly different from that of the normal healthy controls. Our findings on cytokines are also consistent with reports of increased expression of cytokines like IL-8, TNF-α in autoimmune disorders as well as induction of production of cytokines by EBV.[9],[10],[11],[12] In conclusion, our study clearly showed an increased EBV activation among the autoimmune patient groups compared to the normal healthy controls. Further in vitro studies are required to see the association between the aetiology of autoimmune disorders and EBV. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10037t1.jpg] [mb10037t2.jpg] |
| |||||||||
{kind=link}
{kind=link}