 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
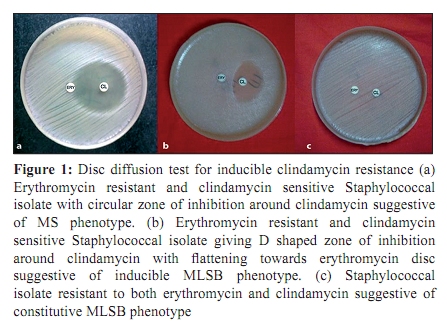
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 124-126 Original Article Inducible clindamycin resistance in Staphylococcus aureus isolated from clinical samples *V Deotale, DK Mendiratta, U Raut, P Narang Department of Microbiology, Mahatma Gandhi Institute of Medical Sciences, Sevagram. Dist Wardha, M.S. - 442 102, India Correspondence Address: *Department of Microbiology, Mahatma Gandhi Institute of Medical Sciences, Sevagram. Dist Wardha, M.S. - 442 102, India, vijayshree_khairkar@rediffmail.com Date of Submission: 08-Jun-2009 Code Number: mb10038 PMID: 20404457 DOI: 10.4103/0255-0857.62488 Abstract Purpose: Clindamycin is commonly used in the treatment of erythromycin resistant Staphylococcus aureus causing skin and soft tissue infections. In vitro routine tests for clindamycin susceptibility may fail to detect inducible clindamycin resistance due to erm genes resulting in treatment failure, thus necessitating the need to detect such resistance by a simple D test on routine basis. Keywords: Clindamycin resistance, constitutive MLS B phenotype, inducible MLS B phenotype, MRSA, MS phenotype Introduction Emergence of methicillin resistance in Staphylococcus aureus has left us with very few therapeutic alternatives available to treat staphylococcal infections. The macrolide-lincosamide-streptogramin B (MLS B ) family of antibiotics serves as one such alternative, with clindamycin being the preferred agent due its excellent pharmacokinetic properties. [1] However, widespread use of MLS- B antibiotics has led to an increase in number of staphylococcal strains acquiring resistance to MLS- B antibiotics. [2] The most common mechanism for such resistance is target site modification mediated by erm genes which can be expressed either constitutively (constitutive MLS B phenotype) or inducibely (inducible MLS B phenotype). Strains with inducible resistance to clindamycin are difficult to detect in the routine laboratory as they appear erythromycin resistant and clindamycin sensitive in vitro when not placed adjacent to each other. In such cases, in vivo therapy with clindamycin may select constitutive erm mutants leading to clinical therapeutic failure. In case of another mechanism of resistance mediated through msrA genes i.e. efflux of antibiotic, Staphylococcal isolates appear erythromycin resistant and clindamycin sensitive both in vivo and in vitro and the strain does not typically become clindamycin resistant during therapy. [3] This study demonstrates a very simple method of detecting inducible resistance to clindamycin in erythromycin resistant staphylococcal isolates. i.e. D test as described by Fiebelkorn et al. [1],[4] Materials and Methods The study was conducted from February to May 2008. A total of 247 isolates of Staphylococcus aureus isolated from various clinical specimens like pus, wound swab, aspirates, blood, and sterile fluids were tested. The isolates were first identified as S. auerus by standard biochemical techniques [5] and then subjected to susceptibility testing by Kirby Bauer's disc diffusion method on Mueller Hinton agar plates using erythromycin (15ìg), penicillin (10U), ciprofloxacin (5 ìg) and cefoxitin (30 ìg) as per CLSI guidelines. Methicillin resistance was detected using oxacillin (1ìg) on Mueller Hinton agar supplemented with 2% NaCl followed by incubation at 350 C. [4] Those isolates which were erythromycin resistant were further subjected to 'D test' as per CLSI guidelines. Briefly, erythromycin (15 ìg) disc was placed at a distance of 15mm (edge to edge) from clindamycin (2 ìg) disc on a Mueller Hinton agar plate previously inoculated with 0.5 McFarland bacterial suspension. Following overnight incubation at 37 0 C, flattening of zone (D shaped) around clindamycin in the area between the two discs, indicated inducible clindamycin resistance [4] [Figure - 1]b. Three different phenotypes were appreciated after testing and interpreted as follows:
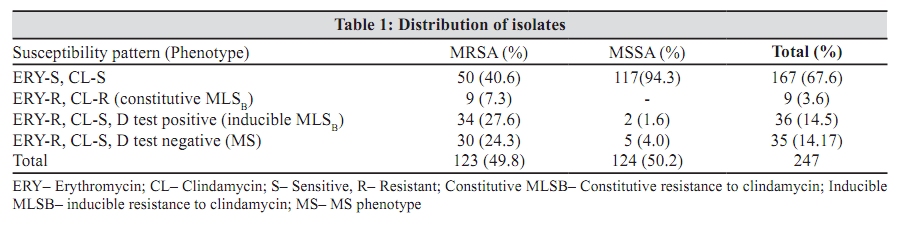
Results Two hundred and forty seven Staphylococcal isolates were tested for susceptibility to erythromycin and other antibiotics of the panel by routine disc diffusion testing; 80 (32.4%) of them were erythromycin resistant. These isolates when subjected to D test showed nine (3.6%) isolates resistant to both erythromycin and clindamycin indicating constitutive MLS B Phenotype; 71 isolates showed clindamycin sensitivity. Out of these, 36 isolates showed positive D test indicating inducible MLS B phenotype while 35 gave negative D test indicating MS phenotype [Table - 1]. The overall percentage resistance for all three phenotypes was as follows. Inducible clindamycin resistance - 14.5% constitutive clindamycin resistance - 3.6% MS Phenotype - 14.17% Percentage of both inducible and constitutive resistance was higher amongst MRSA isolates as compared to MSSA [Table - 1]. Discussion The determination of antimicrobial susceptibility of a clinical isolate is often crucial for optimal antimicrobial therapy of infected patients. This is particularly important considering the increase of resistance and the emergence of multidrug resistant organisms. There are many options available for treatment of MSSA and MRSA infections, with clindamycin being one of the good alternatives. [1] However, clindamycin resistance can develop in staphylococcal isolates with inducible phenotype, and from such isolates, spontaneous constitutively resistant mutants have arisen both in vitro testing and in vivo during clindamycin therapy. [6] Reporting Staphylococcus aureus as susceptible to clindamycin without checking for inducible resistance may result in institution of inappropriate clindamycin therapy. On the other hand negative result for inducible clindamycin resistance confirms clindamycin susceptibility and provides a very good therapeutic option. [7] In our study we found high percentage of erythromycin resistant isolates [80 (32.4%)]. Amongst them 36 (45%) isolates tested positive for inducible clindamycin resistance by D test while rest of the isolates were negative for D test, out of which 9 (11.25%) were shown to have constitutive clindamycin resistance and 35 (43.75%) showed true sensitivity to clindamycin (MS phenotype). These observations suggest that had D test not been performed, nearly half of the erythromycin resistant isolates would have been misidentified as clindamycin sensitive resulting in therapeutic failure. It was also observed that percentages of inducible resistance and MS phenotype were higher amongst MRSA (27.6% and 24.3% respectively) as compared to MSSA (1.6% and 4%). This was in concordance with a few of the studies reported before - Yilmaz et al.[6] found inducible resistance of 24.4% in MRSA and 14.8% in MSSA; Gadepalli et al.[2] showed it to be 30% in MRSA and 10% in MSSA, while Mohamed Rahabar et al.[8] reported 22.6% in MRSA and 4% in MSSA. Another study from India [9] showed very high frequency of inducible resistance (63%) in erythromycin -R, clindamycin sensitive isolates being 74% in MRSA and 45% in MSSA. On the contrary, Schreckenberger et al.[10] and Levin et al.[11] showed higher percentage of inducible resistance in MSSA as compared to MRSA, 7-12% in MRSA and 19-20% in MSSA; 12.5% MRSA and 68% MSSA respectively. Constitutive resistance in our study was seen in 7.3% of MRSA isolates, which is contrary to the only study from India, by Angel et al.,[12] which did not find it in any of the strains,. In the light of the restricted range of antibiotics available for the treatment of methicillin-resistant staphylococcal infections and the known limitations of vancomycin, clindamycin should be considered for the management of serious soft tissue infections with methicillin-resistant staphylococci that are sensitive to clindamycin. [13] The true sensitivity to clindamycin can only be judged after performing D test on the erythromycin resistant isolates. The prevalence of inducible clindamycin resistance may vary from hospital to hospital. Although we did not study the prevalence of inducible clindamycin resistance in our area, from the current study, we can conclude that there is a fairly high percentage of inducible clindamycin resistance amongst the staphylococcal isolates which shows erythromycin resistance. Use of D test in a routine laboratory will enable us in guiding the clinicians regarding judicious use of clindamycin in skin and soft tissue infections; as clindamycin is not a suitable drug for D test positive isolates while it can definitely prove to be a drug of choice in case of D test negative isolates. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10038t1.jpg] [mb10038f1.jpg] |
| |||||||||

{kind=link}
{kind=link}