 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
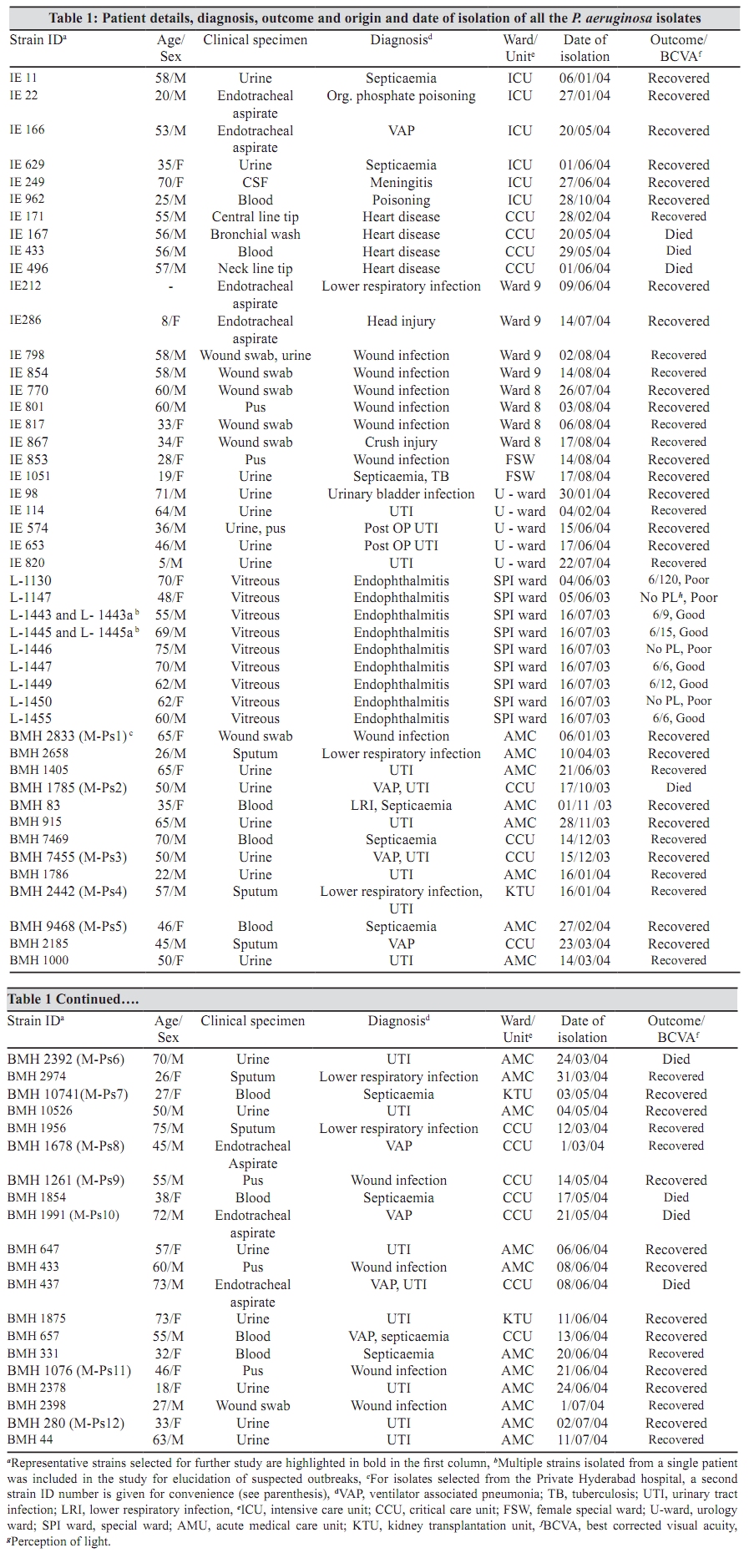
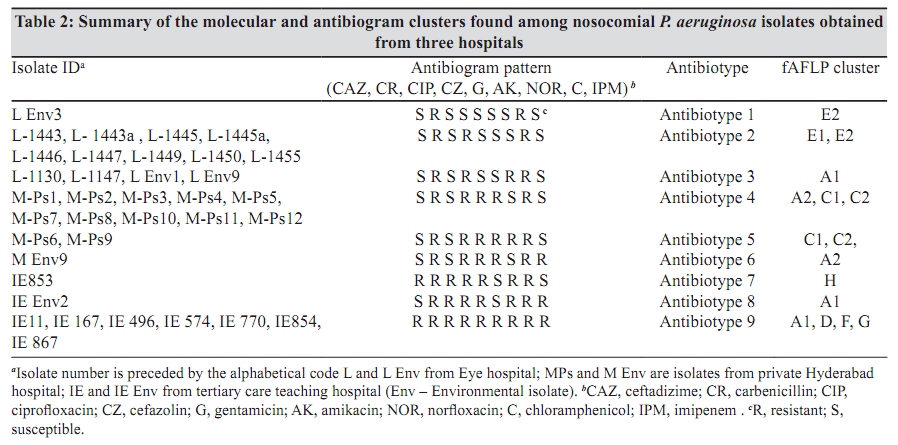
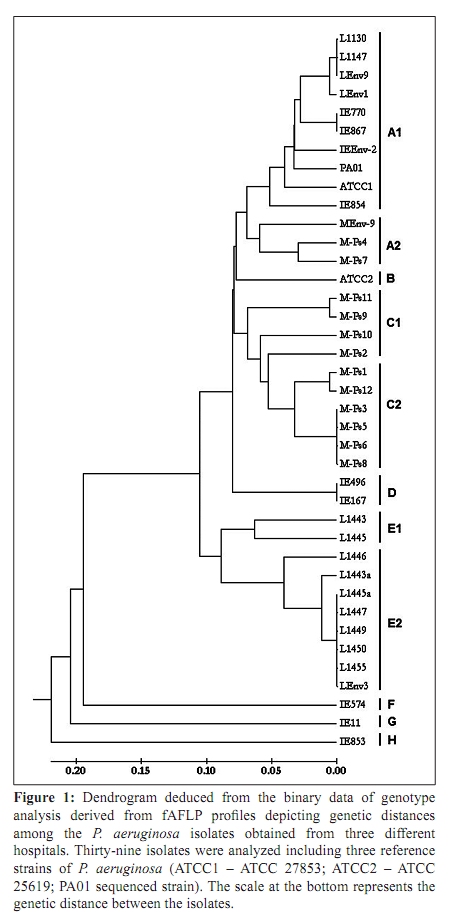
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 130-137 Original Article Correlations between genotyping and antibiograms of clinical isolates of Pseudomonas aeruginosa from three different south Indian hospitals *K Prashanth, SK Singh, R Kanungo, S Sharma, P Shashikala, S Joshi, S Jayachandran Department of Biotechnology (KP, SKS, SJ), School of Life Sciences, Pondicherry University, R. Venkataraman Nagar, Kalapet, Puducherry - 605 014, Department of Clinical Microbiology (RK, PS), Pondicherry Institute of Medical Sciences, Puducherry 605 014, Jhaveri Microbiology Centre (SS), L.V. Prasad Eye Institute, Banjara Hills, Hyderabad - 500 034, Bhagavan Mahaveer Hospital and Research Centre (SJ), AC Guards, Hyderabad 500 004, India Correspondence Address: *Department of Biotechnology, School of Life Sciences, Pondicherry University, R. Venkataraman Nagar, Kalapet, Puducherry - 605 014, India, prashi2k@gmail.com Date of Submission: 30-Jul-2009 Code Number: mb10040 PMID: 20404459 DOI: 10.4103/0255-0857.62490 Abstract Purpose : To compare the molecular relationships and antibiograms of nosocomial isolates of Pseudomonas aeruginosa obtained from three different genres of hospitals located in Southern India, two located at Hyderabad (one private hospital and an ophthalmic hospital) and one in Puducherry (tertiary care teaching hospital). Each of these hospitals, which follow different infection control strategies and various problems associated with it, were investigated. Keywords: fAFLP, infection control practices, multiple-drug resistance, Pseudomonas aeruginosa Introduction Hospital acquired infections in the acute care units are a major threat to patient safety. Pseudomonas aeruginosa is implicated in a wide spectrum of nosocomial infections, including bacteremia, secondary meningitis, wound infection, severe sepsis, ocular and urinary tract infection, [1] but their most important role appears to be as agents of nosocomial pneumonia, particularly ventilator-associated pneumonia (VAP) in patients confined to hospital intensive care units (ICUs). [2] Chronically infected cystic fibrosis patients also known to be colonised by distinct strains of P. aeruginosa. [3] These organisms seem to have a remarkable ability to acquire antibiotic resistance genes, to persist in the hospital environment and to spread easily from patient to patient. [1] Outbreaks of multiresistant P. aeruginosa infection in hospitals with efficient infection control policies may be due to advanced invasive procedures adopted in ICUs. Such situations have also resulted in the dissemination of only a few particular persistent resistant clones in hospitals. [4],[5] Many nosocomial infection surveillances of ICUs have demonstrated that P. aeruginosa is capable of long-term persistence in hospital environments. [1],[6] The present study investigated the molecular relationships and antibiograms of nosocomial isolates of P. aeruginosa from three different hospitals. The Puducherry hospital is a typical tertiary care teaching hospital with approximately 500 beds that caters the need of Puducherry and large geographic area of nearby state Tamil Nadu, while the private hospital is a small acute care hospital located at Hyderabad, state capital of Andhra Pradesh, catering the needs of the city population and is substantially under-resourced for the high number of patients that it serves. Tertiary care teaching Puducherry hospital follows active infection control measures with regular disinfection of clinical areas and periodic surveillance of hospital for resistant bacteria. In private Hyderabad hospital, surveillance of hospital environment and patients for resistant bacteria though performed, it is infrequent and not adhered to regular intervals. Lack of resources has held routine disinfection measures hostage in private Hyderabad hospital. The ophthalmic hospital, Hyderabad, is an ocular specialty hospital admitting only ocular disease patients. The eye hospital has an active infection control committee engaged in active surveillance of nosocomial infections and has exemplary infection control practices that include stringent disinfection procedures. All cases of ocular infections are investigated microbiologically and appropriate records are maintained to trace the source in case of any outbreak. We hypothesise that there will be a difference in strain characteristics isolated from patients and environment when there is difference in kinds of infection control measures followed by the hospitals. The main aim of the present study was to compare the molecular genotyping profiles and antibiogram results of clinical and hospital environmental P. aeruginosa isolates obtained from three different genres of hospitals located at Hyderabad and Puducherry that are following different hospital infection control and surveillance practices. Additionally, the study also correlated the effectiveness of these practices through the analysis of the genotyping results. Comparison of the isolates obtained from three different settings was done by using antibiotyping and whole genome fingerprinting. Antibiotyping was done by disk diffusion method whereas fluorescent amplified fragment length polymorphism (fAFLP) was the genotyping tool. Materials and Methods Bacteria were isolated by clinical microbiology laboratory presumptively identified as P. aeruginosa by standard techniques [7] from patient or environmental samples. They were later confirmed by API 20NE system (bioMérieux, 5, rue des Aqueducts BP 10 - 69290 Craponne, France). A total of 71 P. aeruginosa isolates including five environmental strains were studied from the three hospitals collected during January 2003 to August 2004. Thirty-one representative clinical isolates from this collection were further selected based on distinct antibiotic resistance patterns. In cases where multiple isolates were obtained from the same patient, after performing preliminary biochemical testing and antimicrobial susceptibility testing, a representative strain(s) was selected for further investigation based on their similarity in resistant profiles. Five additional environmental isolates were also included in the study. P. aeruginosa infections in the eye hospital are relatively infrequent, but occasional outbreaks of postoperative endophthalmitis have been witnessed. A collection of nine isolates from the eye hospital from two outbreaks (reported earlier) was included in the study. [8] A total of 23 environmental samples were screened from the operating room environments in the eye hospital yielded three isolates of P. aeruginosa, which were also included in the study. Nine representative isolates were selected from a collection of 24 isolates from tertiary teaching hospital based on their resistance to imipenem (MIC levels), resistograms and the location (ICU/wards) of their isolation. Eight isolates selected had high MIC levels for imipenem ranging from 32 to 128 µg/mL and one isolate was highly susceptible having a MIC of < 1 µg/mL. From acute care unit of private Hyderabad hospital, 12 representative isolates were selected based on their distinct resistance profiles from a total of 33 isolates that were obtained from various P. aeruginosa infections [Table - 1]. In addition, two environmental isolates of P. aeruginosa, one each from tertiary care teaching hospital and private Hyderabad hospital, were also investigated (a total of 80 environmental samples were screened from various clinical areas of each hospital for this purpose). Antimicrobial susceptibility patterns for all the isolates were determined by disc diffusion method [9] on Mueller Hinton agar (Hi-Media, Mumbai) using commercially available paper discs (Hi-Media, Mumbai). The clinical microbiology laboratories of all three hospitals followed same procedure (Clinical Laboratory Standard Institute (CLSI)) for antimicrobial susceptibility testing and used discs only from Hi-media, Mumbai, for consistency. Susceptibility tests were rechecked for reproducibility at our centre, after being checked at respective clinical laboratories of three hospitals. The antibiotics were used in the following concentrations (µg/disc): amikacin (AK), 30; carbenicillin (CR), 100; ceftazidime (CAZ), 30; cefazolin (CZ), 30; chloramphenicol (C), 30; ciprofloxacin (CIP), 5; gentamicin (GEN), 10; imipenem (IPM), 10; norfloxacin (NOR), 10. Plates were incubated at 37°C for 24 hour and inhibition zones were measured from the centre of the disks. These experiments were performed in triplicate and mean of zones of inhibition was derived. Results were interpreted as per the guidelines of CLSI. [9] Isolates showing resistance for imipenem in disk diffusion assay were further tested for determination of MICs for imipenem following the guide lines of CLSI. [9] Molecular relationships between the isolates were determined by Genescan and Genotyper software (Applied Biosystems, Inc., Foster City, CA) analysis of fAFLP profiles generated for all the isolates. [8],[10] For this study, we defined a cutoff of 99.5% similarity (S) as the identity level. [11] Therefore, individual isolates of P. aeruginosa producing fAFLP profiles with S ≥ 99.5% (having ≤0.5% of difference) are likely to be considered as identical clones. Thirty-six isolates along with three standard reference strains (2 P. aeruginosa ATCC strains (ATCC 27853 and ATCC 25619) (Microbios/Himedia, Mumbai) and PA01 (Bangalore Genei, Bengalooru) were characterized by fAFLP as described previously. [8],[10] Using the enzyme combination of EcoRI-MseI, we obtained a fingerprint of approximately 44 fragments distributed within the size range of 50-500 bp. Primer combinations used were EcoRI+0 and MseI+C. The fAFLP experiment and analysis (AFLP Microbial Fingerprinting kit; Applied Biosystems, Inc., [ABI] Foster City, CA) were performed according to the manufacturer's instructions. Analysis of the fAFLP data was performed by construction of dendrograms and visual inspection of the Genescan and Genotyper plots. For construction of the dendrogram, data from all isolates were imported into a Genotyper program for binary matrix creation. The percentage similarities/differences between fAFLP profiles were calculated using the Dice correlation coefficient. The binary data were converted into a distance matrix, and dendrogram was deduced by using the UPGMA (unweighted pair group method with arithmetic mean) algorithm. Results A total of 39 isolates including the three reference strains were investigated in this study. Antimicrobial susceptibility profiles of 36 isolates obtained from the three hospitals showed nine different kinds of antibiograms and they were designated as antibiotype 1 to 9 [Table - 2]. Isolates from each of these three hospitals showed three unique antimicrobial profiles (Eye hospital - antibiotype 1, 2, and 3) (Private Hyderabad hospital - antibiotype 4, 5, and 6), (Tertiary care teaching hospital, Puducherry - antibiotype 7, 8, and 9). Isolates from tertiary care teaching hospital showed more resistant antibiograms wherein isolates were resistant to all the antibiotics tested sparing only ceftazidime, amikacin, and imipenem. Antibiotype 9 from tertiary care teaching hospital, comprising 7 out of 10 isolates showed resistance to all the antibiotics tested including imipenem. Eight isolates from this antibiotype showed high imipenem MIC levels ranging from 32 to 128 µg/mL. Isolates from eye hospital generally showed resistance only to two to four antibiotics notably to carbenicillin, cefazolin, chloramphenicol, and sensitive to all others. Most of the isolates from private Hyderabad hospital were resistant to five commonly tested antibiotics such as carbenicillin, cefazolin, gentamicin, amikacin, and chloramphenicol and susceptible only to ceftazidime, ciprofloxacin, norfloxacin, and imipenem [Table - 2]. A strong similarity in antibiograms (repeatedly checked) among 33 private Hyderabad hospital isolates is one of the criteria used for the selection of isolates for further testing in our study. Eight major clusters were generated for the isolates analyzed through fAFLP genotyping, which were designated alphabetically from A to H [Figure - 1]. Within three major clusters A, C, and E, two subclusters each were also seen (A1, A2; C1, C2; E1 E2). Some clusters consisted of only a single isolate (cluster B, F, G, and H). A1 subcluster comprised more isolates obtained from tertiary care hospital as well as two reference strains (ATCC27853 and PA01) clustered in this group. Major cluster C comprised of only private hospital isolates. Similarly, cluster E had only isolates cultured from eye hospital. Clusters D, F, G, and H comprised only one to two isolates and all these isolates were from teaching hospital. A1 subcluster had isolates from both eye and tertiary teaching hospital. ATCC strain P. aeruginosa (ATCC25619) strain formed a distinct cluster B in the dendrogram. Four isolates belonging to A1 subcluster from eye hospital are indistinguishable as well as six isolates of cluster E were identical. Cluster C2 comprised of four isolates from private Hyderabad hospital, which are also indistinguishable. [Table - 2] provides a list of the resistogram of isolates and summarizes the genotypic and phenotypic characteristics of P. aeruginosa isolated from the three hospitals. Discussion Nosocomial infections in the developing countries pose greater threats to patient safety than in Western countries. In West, the crude mortality rate for patients with device-associated infections ranged from 35.2% (for CVC-associated bloodstream infection) to 44.9% (for VAP) [6] . In India, P. aeruginosa was the commonest species isolated from VAP patients in ICUs (55%) and from wound infections (59%) with high mortality rates ranging from 16% to 46%. [2],[3],[12],[13] Emergence of MDR in P. aeruginosa in many hospitals across the country is of great concern. [3],[13],[14] Although the present study had limitations in number of isolates tested and short duration of screening, multiple resistance among isolates was clearly evident in the study. Almost all the isolates in our study showed resistance to three or more antibiotics. Reports on P. aeruginosa producing β-lactamases have been more frequent from India in recent times, [13] and the increasing number of strains capable of producing extended-spectrum β-lactamase (ESBL) is a worrisome development. Latest study from Vellore, Tamilnadu, has documented the high prevalence (42.8%) of carbapenem resistance in P. aeruginosa isolated from patients with respiratory tract infections in the ICUs. [15] Most of isolates from tertiary teaching hospital showed resistance to carbapenem in this study. High prevalence of aminoglycoside modifying enzymes among the P. aeruginosa isolates in India has also been reported in burns patients. [16] Most recent development is the appearance of metallo-â-lactamase producers among P. aeruginosa.[17] Merely a few studies have employed molecular typing methods like ERIC-PCR and PCR-ribotyping to characterize the P. aeruginosa in India. [3],[18] A recent investigation had employed fAFLP for elucidation of P. aeruginosa isolates obtained from endophthalmitis patients. [8] The present study is not intended to be a formal appraisal of the epidemiological aspects of P. aeruginosa and the associated risk factors, clinical features, and outcomes of infected patients, but instead is meant to assess whether there are differences between the clustering relationships of isolates from three hospitals located in different locations in Southern part of India with differing healthcare infrastructures and infection control practices. In our study, fAFLP genotyping and antibiograms were used to analyze clustering relationships. fAFLP analysis is a PCR-based molecular typing technique that randomly samples a small fraction of the entire genome and has been successfully used in the past to explore endemicity of P. aeruginosa. [19] Patients with MDR P. aeruginosa are at an increased risk for inappropriate empirical antimicrobial therapy, and studies have also demonstrated that delays in appropriate antibiotic treatment may be detrimental to patient outcomes. [1],[20] Nonetheless, antibiotyping has its own advantages in a hospital setting. Since resistance patterns of organisms are often institution-specific, it is imperative that any recommendation for empirical therapy is based on local susceptibility data. Therefore, it is apparent that clinicians practically refer to the institution's antibiogram while selecting antibiotics for empiric use and patient's specific culture susceptibility data for definitive use. In addition, in certain situations antibiograms might be the only practical means by which a small clinical laboratory can attempt to compare the relatedness of isolates. Hence antimicrobial susceptibility results are vital and crucial for any hospital. In this study too, susceptibility results gave key information regarding definite resistance patterns that are unique to a hospital and origin of the isolates. Eleven isolates including environmental isolates from eye hospital (from two independent outbreaks) showed two different molecular clusters similar to the earlier results [8] even while larger number of isolates were included in the clustering analysis. These two clusters comprised of three antibiotypes and were characterized by having more susceptibility profiles. Such susceptibility is quite understandable as most of the isolates causing ocular infections were likely to be endogenous in origin and furthermore they might have cross-contaminated the hospital environments. Environmental strains were indistinguishable from the clinical isolates obtained from eyes in the present study that confirmed the cross-contamination. Isolates from private Hyderabad hospital distributed only in two major clusters, and most of the isolates were resistant to at least four antimicrobials tested. These two clusters of private hospital, appear to be endemic in the hospital causing infections periodically as identical isolates were obtained from different patients and at different intervals.In contrast, isolates recovered from teaching hospital revealed high heterogeneity with five molecular clusters. Furthermore, irrespective of genotypic cluster most of the isolates from teaching hospital showed resistance to all the nine antibiotics tested. Interestingly, cluster A with two subclusters contained isolates from all the three hospitals. Such closely related small number of isolates witnessed in these hospitals presumably indicates higher transmissibility of these isolates in this part of the country. Five environmental isolates obtained from three hospitals showed four kinds of antibiotypes. Environmental isolates were indistinguishable from clinical strains (A1 cluster; antibiotype 3) in eye hospital as demonstrated both by antibiogram and fAFLP. It is also noteworthy that teaching and private hospital environmental isolates were grouped in A1 and A2 subcluster, respectively. A1 had three clinical isolates from tertiary teaching hospital and A2 had two clinical isolates of private hospital, Hyderabad. Private hospital clinical isolates were indistinguishable with environmental isolate MEnv-9 genotypically. These observations advocate more emphasize to be given to cleaner hospital environments to avoid the strain colonization that can form reservoir for future infections. Correlation of different genotypes with the outcome of infection revealed interesting facts. Mortality was mostly due to severe infection by MDR isolates and in all the cases only elderly patients died. Generally infections due to isolates belonging to cluster C and D were responsible for patient's death. Remarkably all the isolates belonged to these two genotypes were multidrug resistant. Similar correlation between mortality and multiple drug resistance was observed by other research workers. [2],[3],[6],[12] Device-related infections due to fAFLP genotype D appear to be more common in the tertiary teaching hospital, which resulted in fatal outcome. While in the small private hospital of Hyderabad, persistent clones of P. aeruginosa belonging to genotypes C1 and C2 mostly causing UTI and VAP were responsible for higher mortality. However, infections due to other genotypes that were mostly susceptible at least for two to three antibiotics were not fatal. Infections caused by P. aeruginosa are particularly problematic because the organism is inherently resistant to many drug classes and is able to acquire resistance to even most potent antimicrobial drugs. [1],[21] The high intrinsic antibiotic resistance of this organism is attributed to factors such as active drug efflux and â-lactamase production.[1],[21],]22] Extensive and increasing use of broad-spectrum antibiotics in India both in community as well as in hospitals located in urban metropolitan cities [23] has served to eliminate competing bacteria and created a vacant ecological niche, which might enhance the ability of particular resistant clones to colonize and subsequently cause infection in susceptible patients. In a private hospital (located in the city), a particular kind of P. aeruginosa clones (cluster C-2) persisted among patients and the hospital environment for long duration, with infections occurring periodically revealing the endemicity of these related isolates probably as a consequence of inadequate infection control measures. In the eye hospital, occasional outbreaks were encountered perhaps as a result of temporary breakdown or lapse in routine infection control measures. Conversely, the prevailing conditions like high throughput of patients in tertiary care teaching hospital located in town makes it difficult to achieve the good standards of infection control. A greater variety of strains seem to have achieved high levels of resistance to a wider range of antimicrobial combinations, possibly as a result of increased indiscriminate use of antibiotics in different kinds of patients (burns unit, trauma, bacteremia, long-stay ICU, and surgical patients). This has resulted in a problematic situation that is difficult to control in which many endemic unrelated MDR P. aeruginosa strains are circulating continuously amongst patients and hospital environment. In many areas of the hospital environment, the varying numbers of infections are likely depended on the stringency of control measures being applied in affected areas at a given point of time. When outbreaks of P. aeruginosa infection occur, it is crucial to determine whether a particular distinct P. aeruginosa strain is involved in outbreak in order to formulate effective infection control strategies. [1],[8] In the eye hospital, identification of the source of infective strain helped us to make rational decisions on sterilization procedures, which halted more cases of infection. [8] Isolates from private Hyderabad hospital were closely related and likely to have common origin as well as endemic in the hospital. Periodic surveillance of patients and the environment has helped in identification of these persistent endemic clones. Suboptimal infection control procedures at private Hyderabad hospital may perhaps have led to such persistence. The superior standards that have been already achieved in certain urban setups (Eye Hospital) also offer a warning of what might result if such procedures are lowered. Hospitals located at rural and town landscapes naturally attract patients from near and far off places. For example, in Puducherry's tertiary teaching hospital, most of the patients admitted are from Puducherry town and from vast border villages of neighbouring Tamilnadu State; hence, altogether different infection control strategies may be relevant in view of the pressure due to high patient throughput in this hospital. This is more so, particularly in this tertiary care teaching hospital as it witnessed diverse unrelated endemic isolates. In summary, the contrast in the strain diversity found in the three hospitals reinforces the need for infection control measures which are efficient and sustained. An active infection control program, with periodic surveillance of infection and hospital environment, can effectively implement the guidelines for prevention to improve patient safety. In addition, stringent antibiotic policies and resistance surveillance programs should be made mandatory, which will assist in implementing infection control measures. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10040f1.jpg] [mb10040t2.jpg] [mb10040t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}