 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
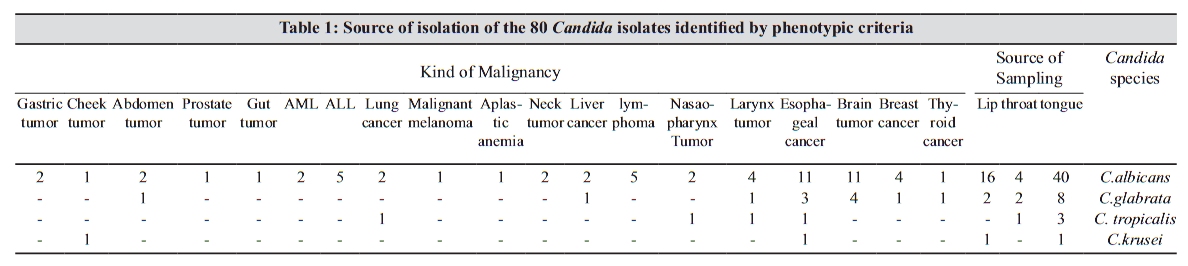
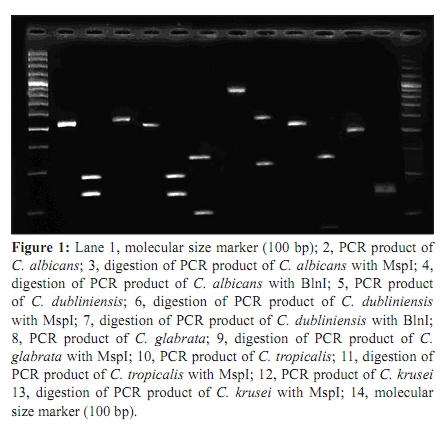
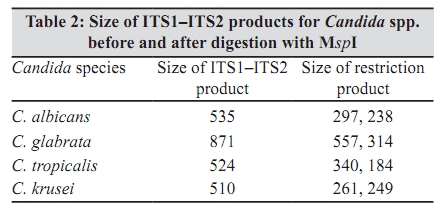
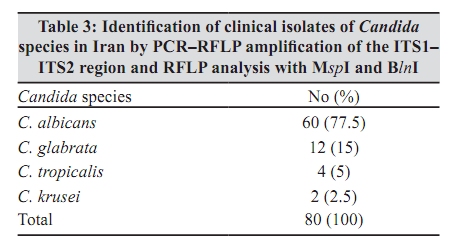
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 147-151 Original Article Identification of Candida species using PCR-RFLP in cancer patients in Iran T Shokohi, MB Hashemi Soteh, Z Saltanat Pouri, MT Hedayati, S Mayahi Department of Medical Mycology and Parasitology (TS, ZS, MTH, SM), Department of Biochemistry and Genetics (MHS), Sari Medical School, Mazandaran University of Medical Sciences, Sari, Iran. Correspondence Address: Department of Medical Mycology and Parasitology, Sari Medical School, Mazandaran University of Medical Sciences, Sari, Iran, shokohi.tahereh@gmail.com Date of Submission: 17-Aug-2009 Code Number: mb10043 PMID: 20404462 DOI: 10.4103/0255-0857.62493 Abstract Opportunistic infections caused by Non-Candida albicans. have been increasing. Traditional methods that are used to identify clinical isolates of Candida species are time-consuming and not appropriate for rapid, accurate and reliable identification.Purpose: To identify Candida spp isolated from cancer patients using PCR-restriction enzyme. Materials and ethods: Using universal primers, ITS1 and ITS4, in this study, we could amplify ITS1-5.8S-ITS2 rDNA regions at both 80 clinical isolates and 3 standard strains. The PCR products were digested with two restriction enzymes MspI and BlnI separately. Result: We successfully identified all isolated species using two restriction enzymes (MspI, BlnI). Candida albicans was the most common species (77.5%), followed by C. glabrata (15%), C. tropicalis (5%), C. krusei (2.5%). Although the primers and enzyme had the ability to identify C. parapsilosis, C. guilliermondii, C. dubliniensis, present isolates did not include these among identified ones. Conclusion: RFLP-PCR using ITSI and ITS4 primers and restriction enzyme is a rapid, easy, reliable and also applicable method in clinical laboratory for identification of medically important Candida spp. Keywords: BlnI, Candida, identification, ITS region, MspI, RFLP-PCR Introduction Opportunistic fungal pathogens are becoming increasingly important causes of both community - acquired and nosocomial infections. The most important fungal pathogens are yeast species belonging to the genus Candida. [1] In recent years, despite advances in therapeutic methods and health care, the incidence of invasive systemic mycoses has increased markedly. This is thought to be the result of the increase in size of populations at risk such as, cancer patients, HIV-infected patients, transplant recipients and those receiving immunosuppressive and broad-spectrum antibiotic therapy. Although Candida albicans remains the most frequent cause of Candidiasis, the incidence of the disease caused by other species of Candida has been increasing steadily. [1],[2] Azoles antifungal agents have therapeutic activity against different Candida spp. Among the azoles drugs, fluconazole shows that satisfactory tolerance has appeared and antifungal drug resistance is quickly becoming a major problem especially in immuno-compromised patients. [3],[4] This resistance also favors the emergence of C. krusei and C. glabrata. [5] As epidemiology, virulence and antifungal susceptibility often vary among strains, a rapid and accurate identification of the species causing the disease is crucial for treatment and epidemiological studies. Early diagnosis of invasive fungal infections is essential to reduce the mortality rates. [6] Current fungal identification methods, including biochemical analysis, germ-tube examination, chlamydospore examination on rice infusion- tween 80 agar and evolution of colonial morphologies on chromogenic agar, represent conventional and reliable approaches; however, these routine methods may require 48 to 72 h or longer in order yielding. Definitive identifications, leading to significant delays in appropriate patients' management due to the significant morbidity and mortality are associated with invasive Candida infections. [7] Given the many limitations of phenotyping methods, molecular biology methods have been adapted because of their ability to detect extremely earlier detection of fungal pathogens, allowing earlier initiation of antifungal therapy and perhaps improved chance of survival. [6] Polymerase chain reaction (PCR) technology can directly detect the presence of fungi with high level of sensitivity and specificity. [8],[9] In this study, we present a PCR-restriction enzyme for discrimination of clinically important Candida spp isolated from patients with cancer. Materials and Methods Eighty strains of Candida spp. and three standard strains (C.albicans, CBS 562; C. glabrata CBS 138; C. dubliniensis CBS 7987) obtained from CBS (Centraalbureau voor Schimmelcultures, Utrecht, The Netherlands) were evaluated for molecular relatedness using RFLP technique. The clinical strains were isolated from, lip, throat and tongue of patients with cancer in four university hospitals, Mazandaran Province [Table - 1]. These strains were previously identified by phenotypic methods such as: color of colony on CHROMagar Candida medium (CHROMagar Company, Paris, France), germ-tube formation in horse serum, chlamydospore formation and sequencing for D1/D2 region of LSU rDNA gene. [10] These samples were cultured on Sabouraoud's dextrose agar (LAB M, Bury, UK) and incubated at 32ºC for 48 h. One colony on each plate was selected and sub-cultured for genotyping. DNA Extraction: Genomic DNA was extracted, using the method of glass bead disruption, [6],[11] PCR Conditions: PCR amplification of ITS1-5.8S-ITS2 rDNA regions was achieved using the ITS1 (forward, 5¢-TCC GTA GGT GAA CCT GCG G-3¢ and ITS4 (reverse, 5¢-TCC TCC GCT TAT TGA TAT GC-3¢) primer pairs (MWG-Biotech AG, Germany). To amplify ITS domains, PCR amplification was performed in a final volume of 50 ìl. Each reaction consists of 2 µl template DNA, 0.5 µl of each primers at 25 µM, 1.25 µl of dNTP (BIORON GmbH, Germany) at 5 mM, 0.5U Taq DNA polymerase (Roche Diagnostics GmbH, Mannheim, Germany) and 5 µl 10× PCR buffer. The amplification parameters consist of 35 cycles of denaturation at 94°C for 1 min, primer annealing at 56°C for 1 min, extension at 72°C for 1 min. In the first cycle, the denaturation step was 94°C for 5 min and in the final cycle the final extension step was 72°C for 7 min. Amplified products were visualized by 1% agarose gel electrophoresis in TBE buffer (20 mmol/l EDTA, 10 mmol Tris boric pH 8). Gel was stained with ethidium bromide (0.5 µg/ml) and photographed by ultraviolet photography. Restriction Enzyme analyses: ITS1-5.8S-ITS2 rDNA regions sequences of several Candida spp. from NCBI's GenBank and D1/D2 region of LSU rDNA regions sequences of some Candida spp. from our previous research [10] were obtained. The restriction sites of various restriction enzymes were determined by CLC workbench software (version 3) and the enzymes (MspI and BlnI; Roche diagnostics, Swiss) were selected. The enzymes were similar to Mirhendi et al. [2],[6] Digestion was performed by incubating 8.5 µl of PCR products that obtained by ITS1 and ITS4 primers with 0.5 µl of each enzymes at 10 U in a final reaction volume of 10 µl at 37ºC for 3 h. Restriction fragment were separated by 3% agarose gel in TBE buffer for 1 h at 100 V. The gel was stained with ethidium bromide (0.5 µg/ml) and photographed by ultraviolet. The size of DNA fragments determined directly with comparison of molecular size marker and distinct banding patterns which demonstrated in similar studies. Results In this study, we apply a PCR-RFLP for identification of the medically important Candida spp. using the universal primers. Universal primers ITS1 and ITS4 amplified ITS region of investigated Candida spp., 80 clinical isolates and 3 standard strains, successfully. And it yielded a unique PCR product size of approximately 510-879 bp. After that PCR products were digested with both MspI and BlnI separately. MspI makes DNA cleave where there is a CCGG sequence. The digestion of ITS region of Candida spp. by MspI enzyme created two bands for C. albicans, C. glabrata, C. tropicalis and C. krusei [Figure - 1] and [Table - 2]. For C. parapsilosis, the size of the PCR and digestion product was similar. The restriction patterns of each Candida spp. were perfectly specific. Since MspI is not able to discriminate between two morphological similar species, C. albicans and C. dubliniensis, we used another enzyme named BlnI, which makes DNA cleave where there is a CCTAGG sequence. As there is only one break point over ITS region of C. dubliniensis, two fragments have been created. In other hand, since there is no break point over ITS region of C. albicans, only one fragment has been created that has the same size as PCR fragment [Figure - 1]. Furthermore, we successfully identified all isolated species using two restriction enzymes. Candida albicans (77.5%) was the most common species among them followed by C. glabrata (15%), C. tropicalis (5%) and C. krusei (2.5%) [Table - 3]. Although it has been already documented [2],[6] that applied primers and enzymes were able to identify C. parapsilosis, C. guilliermondii and C. dubliniensis, there were no such isolates among all identified ones. Discussion Nowadays, the opportunistic pathogen Candida causes a life-threatening infection especially in immuno-compromised patients. [1] In spite of sanitary cares and treatment methods, incidence of candidiasis has increased markedly. [6] The most of Candida spp. that are involved in invasive candidiasis include C. albicans (62%), C. glabrata (12%), C. tropicalis (7.5%), C. parapsilosis (7.3%), C. krusei (2.7%), C. guilliermondii (0.8%) and C. lusitaniae (0.6%). [12] Although, mostly C. albicans is an agent of Candida infections, incidence of the disease with other species such as C. glabrata and C. krusei that are less sensitive to azoles compounds has increased. [1] No detection of C. parapsilosis in our patients is consistence the fact that it is an exogenous pathogen of skin rather than mucosal surface. We did not identify any C. dubliniensis between all isolates suspected to it. The reason for such dramatic variation in the frequency of Candida spp. in our patients are unclear but may include exposure to azoles, patient age, underlying disease, geographic location, or other, unknown, factors. [12] Since, the virulence of the Candida spp. isolated from different locations is varied, rapid and reliable identification methods are crucial for efficient antifungal treatments. The early diagnosis of invasive fungal infections is necessary for decrease of mortality rate. At present, Candida spp. have been identified by traditional techniques such as germ-tube production and biochemical tests. However, these methods need to purify target organisms that are laborious and time-consuming. Candida identification kits based on assimilation require at least 1-5 days for identification at the species level, yet inaccuracies are always possible. [6] Molecular techniques are good substitute for identification and diagnosis of fungus such as Candida spp., because of high power diagnosis being rapid and easy. This procedure with high discrimination power is used in species diagnosis especially in the epidemiological studies to evaluate route of transmission, as well as to choose appropriate antifungal drugs. Several molecular methods for Candida spp. are currently used. [1],[5],[6],[7],[9],[13] However, due to the lack of a gold standard, the optimal method has not been determined. Previous studies demonstrated that no single approach is adequate. [14] Last decade, various molecular techniques were applied since they have high reliability degree for epidemiological research of various strain of pathogenic yeasts. [9],[14] Among these methods, karyotyping [13],[15] and PCR-based techniques are reliable for most typing purposes. Karyotyping is somewhat laborious and time-consuming. PCR methods provided an opportunity for typing that have rapid turnaround times. [16],[17] PCR methods can detect extremely small quantities of DNA and cause earlier detection of pathogenic fungi and consequently allow earlier beginning of antifungal therapy that may improve chances of survival. These methods can directly detect the presence of fungi with high degree of specificity and sensitivity. [9] There have been reports of several studies using PCR techniques together with restriction digestion enzymes for special identification of species that have also expressed several techniques with universal primers for identification of various fungi. These ITS1 and ITS2 regions are surrounded by 5.8SrDNA gene. These regions are appropriate for diagnosis, identification, taxonomy and phylogeny of fungi, which are medically important. Universal primers are usually used as a beneficial approach for clinical microbiological diagnosis. [8],[9],[16] Several methods, such as RFLP, have been reported to identify different fungi using universal primers. [9] Williams et al, [17] used PCR to amplify the ITS region of rDNA and digested the amplified fragments with three restrictions enzymes. They concluded that eight Candida spp. could be identified on the basis of size and sequence variation. PCR-RFLP method has advantages over other molecular techniques, such as restriction fragment length polymorphism with genomic DNA and electrophoretic karyotyping, in being simple and quick. [17] Irobi et al, [18] used RFLP, the fragment of which is generated from ITS of rDNA to differentiate C. albicans, C. tropicalis, C. dubliniensis and C. krusei from 114 Candida isolates and 65 reference strains. McCullough et al, [19] used two molecular techniques to identify unusual strains of C. albicans and to compare them with standard strains of C. dubliniensis and type I C. stellatoidea. Pinto et al, [20] used universal primers ITS1 and ITS4 for the amplification of ITS1 and ITS2 regions, including 5.8S subunit genes and digested it with eight restriction enzymes. They could easily identify Candida spp. on the basis of size and number of bands. Mirhendi et al, [6] using PCR-RFLP method and fungus-specific universal primers (ITS1 and ITS2) were able to amplify the ITS regions of all yeasts tested, and then PCR amplicons were digested with MspI. Finally they could successfully identify six medically important Candida spp. [6] In this study, we apply a PCR-RFLP method to identify the medically important Candida spp. using the universal primers ITS1 and ITS4 to amplify the ITS1 and ITS2 region and 5.8S in the rDNA gene. These primers have already demonstrated their efficiency. [2],[6] In fact, they could amplify the complete part of ITS1, ITS2 and 5.8S rDNA regions and partial part of 18S and 28S rDNA and too many small fragments about 20-30 bp. Similar to other papers, [2],[6] the same results were obtained by CHROMagar and PCR-RFLP methods in detecting different Candida spp, however in our study a couple of isolate showed different results using CHROMagar due to undetermined color. This finding is a conclusive reason to apply molecular methods for determination and identification of medically important Candida spp. in clinical laboratory. Analysis of RFLP derived from the DNA of Candida spp. has the advantage of being easy, fast and reliable in comparison with the phenotypic method, which is insensitive, lacks reproducibility and standardization and besides have limited availability. [5] In general, it seems that this genotyping system comparing the other molecular system and phenotyping system is a rapid, almost inexpensive and completely valid method for identification of Candida spp. This method is useful for clinical and epidemiological investigation both mucocutaneous and systemic forms Since the methods used in this study are easy to perform and just require standard molecular biology equipment, there is no reason to limit the use of PCR in research laboratory. Another advantage of this method, comparing the other molecular methods, is the speed of species identification. For example, hybridization steps require overnight incubation. [8],[17] Moreover, other studies are not able to discriminate large numbers of isolates that include all the recognized pathogenic Candida spp. In conclusion, this genotyping method has been appraised to identify Candida spp. Williams et al,[17] showed that the results were stable after both repeated sub-culturing and storing the isolate for at least six months. This profile was also recommended as an easy and quick method for discrimination between two morphologically similar species, C. albicans and C. dubliniensis. We did not identify any C. dubliniensis between all isolates suspected to dubliniensis. Inclusion, RFLP-PCR using ITSI and ITS4 primers and restriction enzyme is rapid, easy, reliable and also applicable method in clinical laboratory for identification of medically important Candida spp. Acknowledgement We are grateful to the Vice Chancellor of research from Mazandaran University of Medical Sciences for providing financial support. We would like to thank Dr Badali for providing yeast strains from Centraalbureau voor Schimmelcultures (CBS). References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10043t1.jpg] [mb10043t3.jpg] [mb10043t2.jpg] [mb10043f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}