 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
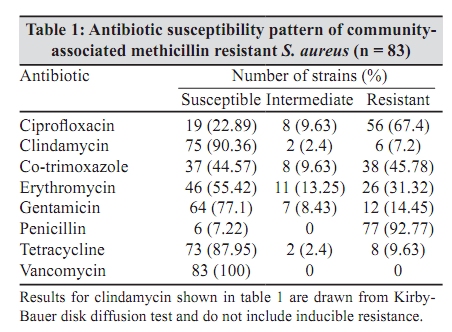
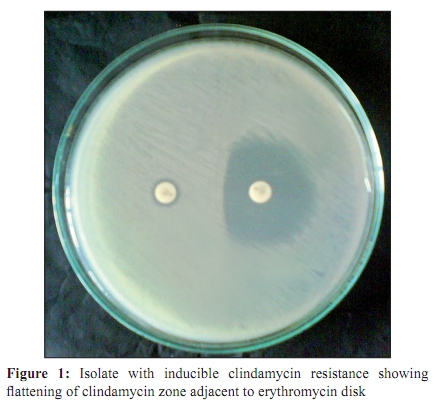
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 152-154 Brief Communication Significance of MRSA strains in community associated skin and soft tissue infections MS Shenoy, *GK Bhat, A Kishore, MK Hassan Department of Microbiology, Kasturba Medical College, Mangalore - 575 001, India Correspondence Address: *Department of Microbiology, Kasturba Medical College, Mangalore - 575 001, India, gkbhat61@yahoo.co.in Date of Submission: 27-Apr-2009 Code Number: mb10044 PMID: 20404463 DOI: 10.4103/0255-0857.62494 Abstract The study was conducted to determine the antibiotic susceptibility profile of community-associated methicillin resistant Staphylococcus aureus (CAMRSA) strains isolated from infections. S. aureus strains were isolated from clinical specimens using the standard procedures. CDC definition was used to classify CAMRSA. Antibiotic susceptibility test was done using Kirby-Bauer disk diffusion method. Double disk diffusion method (D-test) was used to detect inducible macrolide, lincosamide and streptogramin B resistance (inducible MLS B resistance ) . A total of 83 CAMRSA were isolated from abscesses and other skin infections in persons without known risk factors for MRSA infection. All CAMRSA were susceptible to vancomycin. Out of 83 CAMRSA, 13 (15.65%) were D-test positive (inducible MLS B positive) and 6 (7.23%) were positive for constitutive MLS B resistance. Eight strains (9.63%) were resistant to tetracycline and 26 (31.32%) strains were resistant to erythromycin. Increased rate of inducible clindamycin resistance among CAMRSA indicates the importance of identification of such strains by D test to avoid treatment failure when clindamycin is used.Keywords: Community-associated MRSA, D test, inducible clindamycin resistance Introduction Methicillin-resistant Staphylococcus aureus (MRSA) has been recognized as an important nosocomial pathogen worldwide because of the increased rate of multidrug-resistant strains among hospital-acquired MRSA (HAMRSA). Since 1990s, many cases and outbreaks of infections caused by community-acquired MRSA, also been referred to recently as community- associated MRSA (CAMRSA), have occurred. [1] CAMRSA strains usually cause skin and soft tissue infections, but can also cause serious systemic infections such as pneumonia and fasciitis. [2] The epidemiological, clinical, molecular and antibiotic resistance profiles of CAMRSA are distinct from HAMRSA strains. [3] In contrast to HAMRSA, CAMRSA infections often occur in immunocompetent persons without MRSA risk factors, have a type IV staphylococcal cassette chromosome mec (SCC mec) genetic element that encodes for mecA gene, tend to be susceptible for non β-lactam antibiotics and contain pvl gene encoding for Panton-Valantine leukocidin. There are reports of antibiotic resistance in CAMRSA from other countries. [4],[5] Literature search did not give much data on antibiotic resistance of CAMRSA in South India. The objective of this study is observation of inducible macrolide-lincosamide-streptogramin B (MLS B ) resistance utilizing D test apart from determination of antibiotic susceptibility profile of CAMRSA isolated from lesions of patients residing in and around Mangalore, South India. Material and Methods Pus and exudates were collected from patients with skin and soft tissue infections. Demographic and other relevant information was collected. The clinical specimens were inoculated on blood agar and MacConkey's agar, incubated at 37ºC for 24-48 hours and examined for bacterial growth. S. aureus was identified using standard methods based on colony morphology, gram stain, catalase test, mannitol fermentation and coagulase test. [6] Methicillin resistance was detected using cefoxitin disk (30 ìg) diffusion and agar screen method (Mueller-Hinton agar with four per cent NaCl and six ìg oxacillin per ml). Incubation temperature of 37ºC and 35ºC were used in cefoxitin disk and agar screen methods respectively. MRSA was considered community-associated (based on CDC definition) if isolated from infection in persons who were not hospitalized nor had any medical procedure within the past one year and did not receive any antibiotic during the previous two months or identified within 48 hours of hospitalization. The antibiotic susceptibility test was done using Kirby-Bauer disk diffusion method and interpretation was based on CLSI guidelines. [7] Antibiotics (Hi Media Pvt. Ltd, Mumbai) used were - ciprofloxacin (five ìg), clindamycin (two ìg), co-trimoxazole (25 ìg), erythromycin (15 ìg), gentamicin (30 ìg), penicillin (10 u), tetracycline (30 ìg) and vancomycin (30 ìg). S. aureus ATCC 25923 was used for quality control. Inducible MLS B resistance was detected using double disk diffusion test (D-test). [8] Lawn culture of CAMRSA was prepared on Mueller-Hinton agar plate. A 15 ìg erythromycin disk and two ìg clindamycin disks were placed at a distance of 15 mm (edge to edge). The plates were incubated at 35º C for 18 hours and the zones of inhibition were measured and examined to detect flattening of the shape of clindamycin zone facing erythromycin disk (D zone). CAMRSA strains positive in D-test were considered inducible MLS B resistant, strains that were resistant to both erythromycin and clindamycin were considered constitutive MLS B resistant and strains that were resistant to erythromycin but susceptible to clindamycin were considered MLS B phenotype. Results A total of 83 strains of CAMRSA were isolated from abscess and folliculitis. Most CAMRSA strains (25) were isolated from patients of age group 21-30 years, followed by 11-20 years (20), 0-10 years (18), 31-40 years (13) and 41-50 years (seven). None of the patients had MRSA risk factors. The antibiotic susceptibility pattern of CAMRSA is shown in [Table - 1]. None of the isolates were resistant to vancomycin whereas most (92.8%) were resistant to penicillin. Out of 83 strains, six (7.23%) were constitutive MLS B resistant, 13 (15.65%) were inducible MLS B resistant (inducible clindamycin resistant) [Figure - 1] and 13 (15.65%) belonged to MLS B phenotype. Forty six (55.42%) strains were susceptible to both erythromycin and clindamycin. Regarding other antibiotics, 87.95% of CAMRSA were susceptible to tetracycline and 44.57% to co-trimoxazole. Discussion The present study showed the significance of MRSA strains in community associated skin and soft tissue infection. The results are comparable to previous studies. [9],[10] CAMRSA infection can occur in immunocompetent persons with no MRSA risk factors. We observed that 87.95% strains of CAMRSA were susceptible to tetracycline. Tetracycline is not commonly used in treatment of staphylococcal infection and this could be responsible for higher susceptibility of staphylococci to tetracycline. Simple skin infections respond to topical treatment, incision and drainage. However, more serious infections caused by CAMRSA require antibiotic treatment. Erythromycin, co-trimoxazole, tetracycline and clindamycin are the choices. Though clindamycin is absorbed well in the intestine and has good tissue penetration, property development of resistance could be a problem. Methylation of adenosine residue of bacterial 23s ribosomal RNA is the most common mechanism of acquired resistance to macrolides (i.e. erythromycin), lincosamides (i.e., clindamycin) and streptogramin B and confers cross resistance to all MLS B antibiotics. [11] Expression of MLS B resistance in staphylococci is either constitutive or induced. When it is constitutive, staphylococci are resistant to all MLS B antibiotics that can be detected by routine disk diffusion method of antibiotic susceptibility test. In case of inducible MLS B resistance, the bacteria are resistant to erythromycin but susceptible to clindamycin in routine antibiotic susceptibility test. Double disk diffusion or D-test should be used to detect this. Further, erythromycin is an effective inducer of MLS B resistance. Such MRSA strains can potentially develop resistance to clindamycin during therapy. Susceptibility to penicillin in six strains could be due to absence of β-lactamase. It is known that in normal conditions PBP2a may not be expressed. However, all MRSA strains should be considered resistant to penicillin irrespective of test results. The rate of inducible clindamycin resistance in CAMRSA isolates worldwide varies from 2-8 to 94%. [12],[13] In a previous study, 86% of the CAMRSA showed inducible clindamycin resistance while 14% were susceptible to both erythromycin and clindamycin. [14] In the present study, the rate of inducible clindamycin resistance was 15.65%. These studies indicate that inducible MLS B resistance is a problem that needs attention. Teracycline and co-trmoxazole are used for treatment of skin infections caused by CAMRSA. [15] The present study also showed that tetracycline and co-trimoxazole and clindamycin played a role in the treatment of skin and soft tissue infections caused by CAMRSA. The treatment of the patients was based on antibiotic susceptibility test results. D test should always be done on CAMRSA strains to detect inducible clindamycin resistance. In conclusion, increased rate of inducible clindamycin resistance among CAMRSA indicates the importance of identification of such strains by D test to avoid treatment failure when clindamycin is used. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10044t1.jpg] [mb10044f1.jpg] |
| |||||||||
{kind=link}
{kind=link}