 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
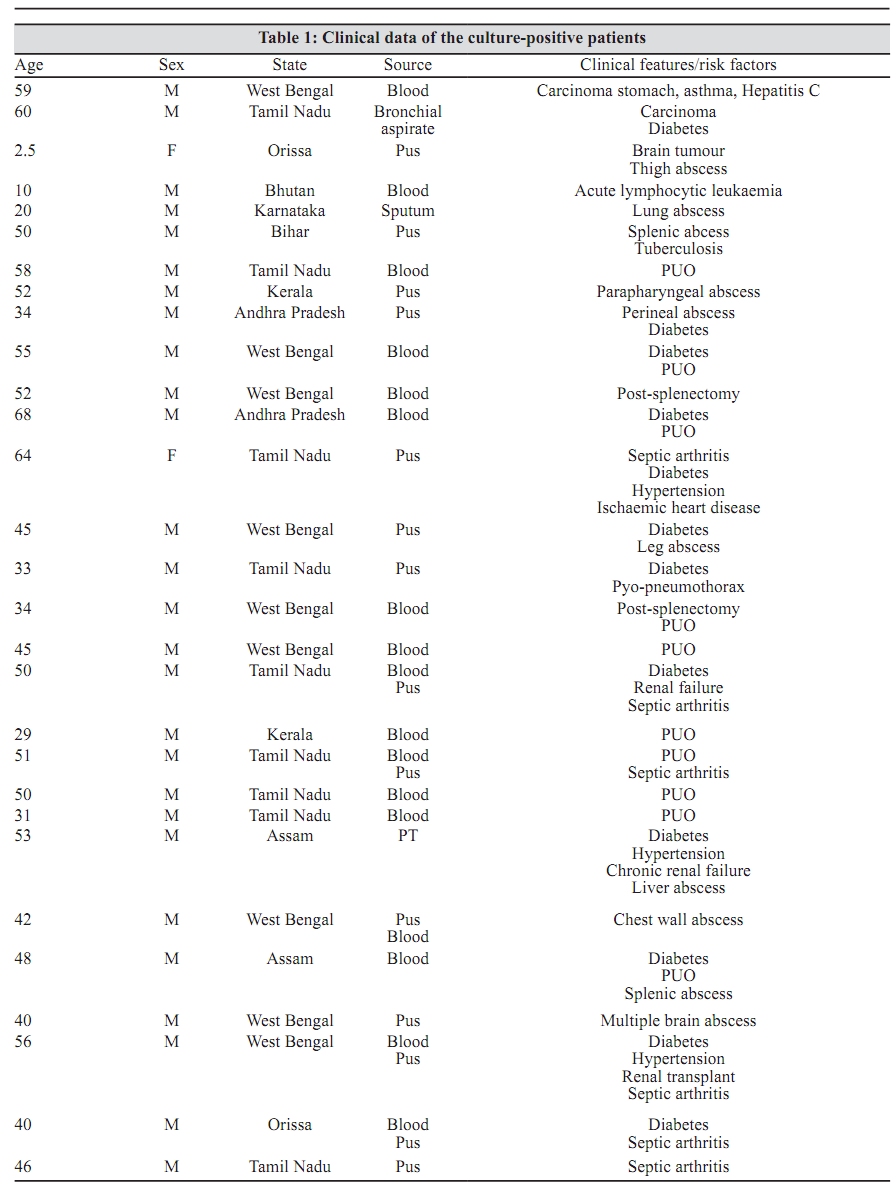
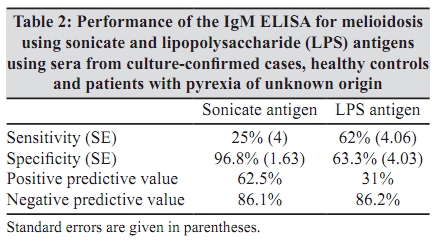
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 158-161 Brief Communication Evaluation of IgM ELISA using a sonicate and a lipopolysaccharide antigen for the serodiagnosis of melioidosis *S Anandan, A Augustine, E Mathai, MV Jesudason Department of Microbiology, Christian Medical College, Vellore - 632 004, India Correspondence Address: *Department of Microbiology, Christian Medical College, Vellore - 632 004, India, shalinianandan@cmcvellore.ac.in Date of Submission: 23-Aug-2009 Code Number: mb10046 PMID: 20404465 DOI: 10.4103/0255-0857.62496 Abstract Melioidosis, caused by Burkholderia pseudomallei, has variable manifestations. The disease can present as an acute or a chronic form or localized or disseminated or can remain latent for many years. Acute septicaemic melioidosis has a high fatality rate when untreated and therefore, an early diagnosis is critical. Lack of testing facilities and of an awareness of the manifestations of the disease makes it likely that it is underreported in India. A sonicate and a lipopolysaccharide (LPS) antigen were evaluated by an IgM enzyme immunoassay in patients with culture-confirmed melioidosis (n = 29), fever of unknown origin (n = 214) and healthy controls (n = 109). Patients with melioidosis had significantly higher optical density values than both control categories, but the sensitivity of both tests was low (25% for sonicate, 62% for LPS). These data highlight the problems with serodiagnosis in endemic settings, where high cut-off values are required for specificity, and result in low sensitivity.Keywords: Burkholderia pseudomallei, IgM, LPS, melioidosis, sonicate antigenIntroduction Introduction Melioidosis, caused by the Gram-negative organism Burkholderia pseudomallei, has variable manifestations. It can present as an acute or a chronic form. Acute lung infection either as a pneumonia with or without pleural involvement is commonly seen, as is acute septicaemia. Skin and soft tissue infections are also a common manifestation and may result in systemic infection from haematogenous spread. [1] The disease is also known to remain dormant for long periods of time, and often when there is a decrease in host immunocompetence such as diabetes mellitus, renal failure, systemic lupus erythematosus or liver disease, the patient presents with symptoms of the disease. In south-east Asia and northern Australia it is a common cause of septicaemia. Relapses are also known to occur., There have been numerous reports from India but limited availability of confirmatory tests makes it possible that this disease is underreported. [2],[3] Acute septicaemic melioidosis has a high fatality rate when untreated or undertreated and in one case series from India has been reported to be 58%. [4] However, the prognosis is good with appropriate and early antibiotic therapy, highlighting the importance of an early diagnosis. [4],[5] Culture is slow, and hence a range of assays, using IgG and IgM responses, have been developed to evaluate the immunologic response. Assays detecting antibodies to B. pseudomallei include indirect haemagglutination (IHA), an indirect fluorescent antibody (IFA), enzyme-linked immunosorbent assays (ELISAs) and immunochromatographic tests. [5] The antigens used include a cell extract, veronal extract, culture filtrates, sonicates, various other antigens like a 19.5 kDa, 39.0 kDa and 200 kDa exopolysaccharide immunoaffinity-purified antigen and lipopolysaccharide (LPS). [5],[6],[7] The range of techniques and antigens applied indicate the difficulty in the identification of a single method or antigen for serological diagnosis of melioidosis. This study was undertaken to establish the prevalence of antibodies to B. pseudomallei in a population of patients and also to strengthen the existing facilities for the diagnosis of melioidosis. We report the evaluation of sonicate and LPS antigens in IgM ELISAs in patients with culture-confirmed melioidosis. Materials and Methods Subjects After obtaining approval from the institute's research and ethics board, serum samples were collected from (1) healthy controls: apparently, healthy individuals at routine pre-employment or antenatal check-up (n = 109); (2) culture-proven cases: patients with blood, pus, joint fluid or sputum cultures positive for B. pseudomallei (n = 29) and (3) pyrexia of unknown origin (PUO): patients with fever in whom tests for tuberculosis, malaria and typhoid and the febrile agglutination tests were negative (n = 214), over a 3-year period. Preparation of the sonicate antigen The antigen was prepared from five strains of B. pseudomallei (confirmed by the Centre for Infections, Health Protection Agency, Colindale, London) as described by Ashdown et al. [8] The working concentrations of the antigen diluted in a carbonate buffer, pH 9.6, and serum were determined by checkerboard titration. Preparation of the LPS antigen The antigen was prepared by the hot-phenol extraction method as previously described. [9] Checkerboard titration was used to optimize the concentration of the antigen and was used at 1:30, diluted in the carbonate buffer, pH 9.6, and serum in 1:200 dilution. IgM ELISA using the sonicate or LPS antigen Flat-bottom 96-well plates (FALCON or Tarson) were coated with 100 ìl sonicate or LPS antigen and incubated overnight at 4° C in a moist chamber. The plates were washed thrice with phosphate buffered saline (PBS), pH 7.4, containing 0.05% (vol/vol) Tween 20 (PBS-T) and blocked with 150 ìl 5% skimmed milk in PBS (for sonicate) or 1% bovine serum albumin (HiMedia) in PBS (for LPS), in a moist chamber at 37° C for 60 min. The plates were washed three times with PBS-T and dried by blotting. Antigen, reagent and calibrator controls (positive samples with known OD values) were included with every run. Each test serum was assayed in duplicate, using 100 µl of 1:500 (for sonicate) or 1:200 (for LPS) dilution in PBS-T, incubated at 37° C for 60 min. After three washes with PBS-T, 100 ìl of the horseradish peroxidase-conjugated rabbit antibody to human IgM (Dako), diluted 1:3000 in PBS-T, was added to each well and the plates were incubated at 37° C for 60 min. After three washes with PBS-T, 100 ìl o -phenylenediamine (OPD, Dako) substrate was added to each well. The plates were incubated in the dark at room temperature and the reaction was stopped after 30 min by addition of 100 ìl 0.5 M H2 SO 4 to each well. The plates were read at 492 nm. Statistical analysis The statistical analysis was performed using SPSS v9. The mean +2 SD of the healthy controls was used to obtain the cut-off value. The Mann-Whitney U-test was used to compare the OD values of the three groups. Inter-group comparisons and statistical significance were tested using Student's t-test and the chi-square test. Results The clinical and epidemiological data of the 29 culture-proven patients with melioidosis are presented in [Table - 1]. IgM ELISA using the sonicate antigen Culture-confirmed cases had a mean OD of 0.77 (SD 1.00), which was significantly higher than the ODs of controls (OD 0.27, SD 0.34) and patients with PUO (OD 0.25, SD 0.43) (P < 0.001). There was no significant difference between the mean OD obtained among healthy controls and those with PUO. Using a cut-off of 0.95 based on mean + 2SD of healthy controls, we found that only 2.9% and 2.1% of the healthy controls and those with PUO, respectively, were above the cut-off value (P = 0.002 and P < 0.001). However, the test only identified 23.8% of the culture-confirmed cases as positive. Constructing a receiver-operating characteristic (ROC) curve did not identify a better cut-off OD value. IgM ELISA using the LPS antigen Culture-confirmed cases had a mean OD of 1.44 (SD 0.89), which was significantly higher than the ODs of the controls (OD 0.84, SD 0.46, P = 0.001) and patients with PUO (OD 1.00, SD 0.60, P = 0.01). There was no significant difference between the mean OD obtained among healthy controls and those with PUO. As the OD values did not follow a normal distribution, an ROC curve was plotted to obtain the cut-off of 1.01. Using this cut-off value, 62.0% cases were positive, as compared to 36.6% and 40.6% of the healthy controls and those with PUO (P = 0.013 and P = 0.028). The accuracy indices of both tests are shown in [Table - 2]. Discussion It is crucial to make an early diagnosis in melioidosis as the mortality rate is high. [4] The diagnosis of melioidosis is made by clinical evaluation and by the recovery and correct identification of B. pseudomallei from cultures of clinical specimens, which remains the 'gold standard' for laboratory diagnosis. However, because of the wide spectrum of disease presentations, if cultures for B. pseudomallei are negative, melioidosis poses diagnostic and therapeutic challenges. In addition, bacteriological culture methods are time-consuming, and the result is often too late to be of use in deciding on or modifying treatment. Thus, serological methods would be of tremendous help in the early diagnosis and timely treatment, and therefore decrease the mortality of melioidosis. The performance of the IgM ELISA has been evaluated in several studies using different antigens. These assays had a sensitivity ranging from 63.5% to 93% and a specificity from 81.8% to 99%. [8],[9],[10],[11] The IgM class of antibodies are frequently used for diagnosis in acute infections, but in endemic areas with frequent exposure and high background seropositivity, such as south-east Asia and India, the diagnostic utility of a serological test is reduced. [1],[12] In this study, an ELISA for the detection of IgM antibodies to B. pseudomallei in serum was standardized and evaluated using two different antigens, of B. pseudomallei, a sonicate and a lipopolysaccharide antigen. Despite the good specificity, the sensitivity of the IgM ELISA was low. This was probably due to the fact that clinically melioidosis can present as a chronic disease with an acute-on-chronic picture. This suggests that the clinical course of a majority of patients with melioidosis may start several days or weeks before they seek medical help, thus allowing time for the development of IgG antibodies and for IgM antibodies to decline. The sensitivity of the test system could be improved by using characterized immunity-affinity purified antigens or well-defined specific antigen fractions. [11] A high negative prediction was exhibited by both assay systems; hence the tests could be used in conjunction with an IgG ELISA, which is more sensitive and specific. In our study, an ELISA using the sonicate antigen was easy to perform and had a high specificity. Thus a negative test could support a decision not to initiate specific therapy especially in a situation where culture facilities are unavailable and/or delayed. In a similar study done in our institution, the IgG ELISA was standardized and evaluated using the sonicate antigen and was found to have a sensitivity of 83.3%. [13] A combination of the IgM and IgG ELISA using the sonicate antigen may be used in the early diagnosis of melioidosis, facilitating early treatment. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10046t2.jpg] [mb10046t1.jpg] |
| |||||||||

{kind=link}
{kind=link}