 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
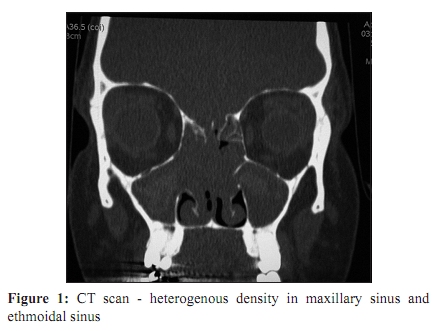
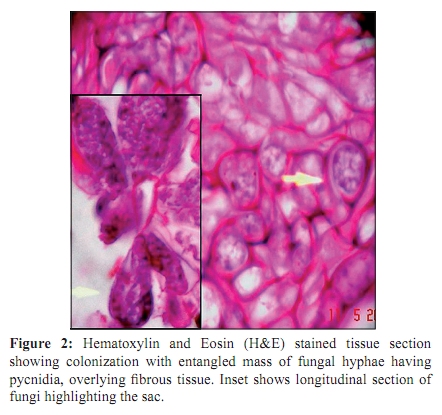
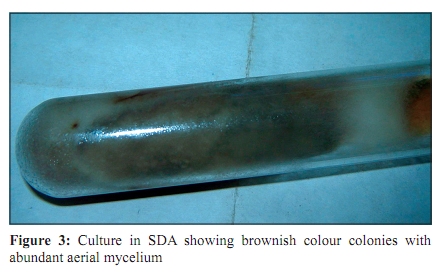
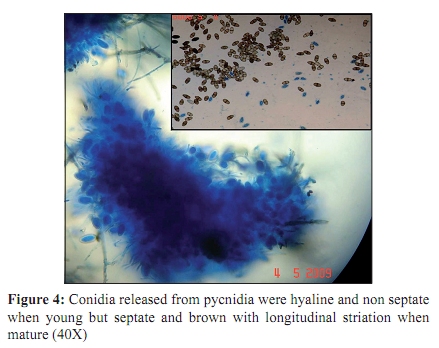
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 167-169 Case Report Maxillary sinusitis caused by Lasiodiplodia theobromae *AJ Kindo, Pramod C, Anita S, S Mohanty Department of Microbiology (AJK, AS), Department of ENT (PC, SM), Sri Ramachandra University, Porur, Chennai - 600 116, India Correspondence Address: *Department of Microbiology, Sri Ramachandra University, Porur, Chennai - 600 116, India, anupmalakra@yahoo.com Date of Submission: 19-Jun-2009 Code Number: mb10049 PMID: 20404468 DOI: 10.4103/0255-0857.62499 Abstract Lasiodiplodia (monotypic) comprises a very small proportion of the fungal biota. It is a common plant pathogen in tropical and subtropical regions. Clinical reports on its association with onychomycosis, corneal ulcer and phaeohyphomycosis are available. However, Lasiodiplodia theobromae causing fungal sinusitis has not been reported. We present here a case of fungal sinusitis in a 30-year-old woman, who came to the ENT OPD (out patient department) with complaints of intermittent bleeding and nasal discharge from the left side for a week. The patient complained of headache, predominantly on the left side and heaviness on and off since two months. Diagnosis was based on radiological and mycological evidence; the patient underwent endoscopic surgery and was started on antifungal treatment.Keywords: Fungal sinusitis, immunocompetent host, lasiodiplodia theobromae Introduction Introduction Lasiodiplodia theobromae, the type species of the genus Lasiodiplodia, has a worldwide distribution but is most common in the tropics and subtropics. [1] This particular fungi causing disease in fruiting plants like papaya has been reported in Hawaii and India only; unidentified Botryodiplodia spp. (synonym of Lasiodiplodia theobromae) have been reported from Brazil and Mexico causing papaya stem cankers. [2] Less frequently, it has been associated with keratomycosis and phaeohyphomycosis in humans. [3],[4] This organism causing fungal rhino sinusitis has not been reported. Fungi, which have been considered simple organisms, are extremely adaptable to diverse environmental conditions. They can exhibit striking differences in appearance with temperature changes. Therefore, unless the essential conditions for culture are provided it can be very difficult to accurately speciate a fungus. Case Report A 30-year-woman attended the ENT OPD on April 11, 2009, with complaints of intermittent bleeding and discharge from the left nostril for one week. The patient complained of left sided headache and heaviness on and off since months. There was no history of ear/throat pain or ear discharge. Patient was neither diabetic nor hypertensive. She did not have any history of chronic illness like bronchial asthma or tuberculosis. There was no history of surgery of any kind in the past. On examination, patient was afebrile with pulse rate of 82/min, respiratory rate 20/minute; blood pressure was 110/80mm Hg. All other systems were normal. Local examination of the nose showed no local deformity, vestibules were normal. There was bilateral hypertrophy of the inferior turbinate and the mucosa appeared pale and irregularly thickened with some debris. Bilateral osteomeatal complex (OMP) was blocked. Pus was observed in the left middle meatus. Laboratory investigations showed haemoglobin 11.7 g/dl total count 8310/cumm, plasma glucose of 88mg/dl. CT scan of the paranasal sinuses showed mucosal thickening of the frontal and, sphenoidal sinuses. Maxillary and ethmoidal sinuses, on either side, along with osteomeatal units showed mucosal thickening. Bilateral infundibular widening was seen [Figure - 1]. Radiological diagnosis was: pansinusitis with sinonasal polyposis. The patient underwent endoscopic surgery, left side middle meatal antrostomy, uncinectomy and sphenoidectomy under general anaesthesia. Fungal debris was removed from the maxillary antrum and polyps were removed from all the sinuses in both nostrils. The sphenopalatine artery was cauterized. Clinical specimens were collected and sent to the laboratory. The tissue, after mincing into small pieces, was subjected to 10% potassium hydroxide (KOH) mount which showed narrow septate hyphae. The minced specimen was inoculated into Sabouraud's dextrose agar (SDA) for fungal culture. On SDA, cottony colonies appeared. These became dark grey within seven days [Figure - 2]. Growth at 37°C was more rapid than that at 25°C. Microscopic examination after lactophenol cotton blue staining showed septate brown hyphae with a width of 6 ìm. The mould was also grown on oatmeal agar. Colonies produced hairy, dark brown round to oval structures which could be seen under the stereoscopic microscope which resembled a structure of a pycnidia.[5] Conidia released from the pycnidia were hyaline and nonseptate when young but were septate and brown, with longitudinal striations, when mature [Figure - 3]. The fungus was identified as Lasiodiplodia theobromae.[5] The histopathological report endorsed our findings showing the fibrosed tissue with entangled fungal hyphae with no tissue invasion. Cut section of the pycnidia showed a pear shaped, enclosed structure broad at one end with a narrow opening on the other end containing the conidia [Figure - 4]. Discussion Natural habitat includes many different kinds of plants. Lasiodiplodia (monotypic) comprises of a very small proportion of the fungal biota. It is a common plant pathogen in tropical and subtropical regions. Formerly called Botryodiplodia theobromae, Lasiodiplodia theobromae is a plant pathogen with a very wide host range. It causes rotting and dieback in most species it infects. [2] It is a common post harvest fungus disease of citrus known as stem-end rot. Lasiodiplodia theobromae, is a rare cause of mycotic keratitis, [3] showing characteristic two-celled, pigmented, longitudinally striate pycnidioconidia. L. theobromae is a cosmopolitan, tropical saprophytic coelomycete which forms pycnidia. Known for almost a century, L. theobromae, is the anamorph of Botryosphaeria rhodina a member of the subphylum Pezizomycotina of Ascomycota, and a common plant pathogen in tropical countries. L. theobromae was the only species of Lasiodiplodia known until recently when four additional species were described. These include L. gonubiensis, described in 2004 [6] and L. venezuelensis, L. crassispora, and L. rubropurpurea, described in 2007, based on results from ITS and EF1á sequence analysis and morphology.[7] These novel species are considered very rare and have limited geographic distributions. Human infections with the type species L. theobromae have been extremely rare, though, a case of pneumonia in a liver transplant patient caused by L. theobromae has been reported. [8] Other reports include, onychomycosis, corneal ulcer, and phaeohyphomycosis. [8] In previous cases, infections of the eyes, skin, and soft tissues were believed to be the result of direct inoculation of the fungus. In this patient, the mode of acquisition of the fungus remains enigmatic. Fungal infection of the paranasal sinuses is an increasingly recognized entity in normal and immunocompromised individuals. Aspergillus species are the most common causative agents of fungal sinusitis. Other fungal causes are some of the dematiaceous fungi. Rhinosinusitis caused by L. theobromae is exceptional. The treatment modality for fungal sinusitis in general is surgery with antifungal agent especially in invasive type of fungal sinusitis. The ideal treatment for this fungus is not defined and there is no consensus regarding treatment with a particular antifungal agent. Surgical debridement is an important aspect of treatment for fungal sinusitis. Our patient underwent surgery on April 13, 2009 and was discharged two days later. She was started on tab itraconazole 100mg orally bd (two months) after fungal identification. Patient was asked to come for a follow-up after 15 days and subsequently after a month. The patient was fully relieved of all symptoms and the repeat nasal endoscopy on follow-up showed completely healed mucosa and bilateral patent ostia. Conclusion We have presented a rare fungus (primarily a plant pathogen) causing fungal sinusitis (non invasive type) in a normal healthy individual. It was promptly and successfully treated following clinical suspicion of fungal aetiology with symptoms. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10049f2.jpg] [mb10049f4.jpg] [mb10049f3.jpg] [mb10049f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}