 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
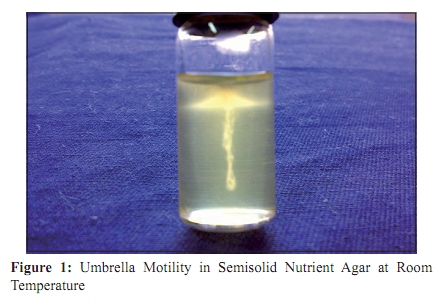
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 169-171 Case Report Listeria monocytogenes meningoencephalitis in an immunocompetent, previously healthy 20-month old female child *MA Peer, RA Nasir, DK Kakru, BA Fomda, MA Wani, QN Hakeem Sher-I-Kashmir Institute of Medical Sciences (SKIMS), Soura, Srinagar, Kashmir, India Correspondence Address: * Sher-I-Kashmir Institute of Medical Sciences (SKIMS), Soura, Srinagar, Kashmir, India, peermaroofhussain@yahoo.com Date of Submission: 27-Jul-2009 Code Number: mb10050 PMID: 20404469 DOI: 10.4103/0255-0857.62500 Abstract Invasive listeriosis predominantly affects pregnant women, neonates, elderly and people with a compromised immune function. For more than 80 years since the discovery of Listeria in 1924, only a few reports of invasive listeriosis in humans have emerged from India, with all of them in patients having an underlying predisposition. We, however, report Listeria monocytogenes meningoencephalitis in an immunocompetent, previously healthy, 20-month-old female child with no underlying predisposition. The patient showed poor response to empirical treatment with vancomycin and ceftriaxone but improved dramatically after substitution with ampicillin and amikacin. She had a complete recovery other than left lateral rectus palsy that persisted.Keywords: Immunocompetent, Listeria monocytogenes, meningoencephalitis Introduction Unlike most other food borne pathogens, which primarily cause gastrointestinal illness, Listeria monocytogenes causes severe invasive syndromes including sepsis, meningitis, meningoencephalitis and rhomboencephalitis. World over, invasive listeriosis is, however, an uncommon cause of illness in the general population, with a particular predilection for affecting pregnant women, neonates, elderly and immunocompromised patients. [1] Recent annual incidences in the United States range from two to nine cases per million population. [2] Over a period of more than 80 years, since the first description of L. monocytogenes infection by Murray et al. in rabbits, only a few cases of invasive listeriosis in humans have emerged from India. [3],[4],[5],[6],[7] However, patients affected in all these studies belonged to high risk groups with a predilection for invasive listeriosis. Though L. monocytogenes may account for 4 to 16% of patients with neonatal sepsis or meningitis, it is very uncommon in immunocompetent children beyond the neonatal period. [8] In the current case, a previously healthy 20-month-old immunocompetent female child with normal developmental milestones had no underlying predisposition. Case Report A previously healthy 20-month-old female child presented to our hospital with two days history of fever, vomiting and refusal to feed. On examination, she was irritable and drowsy, with mild neck stiffness. Her pulse rate was 110 beats/minute, fever 103˚F, RR 28/min and BP 100/60. Rest of the systemic examination was normal. Initial laboratory investigations showed an elevated WBC count of 24080/µl with 69% neutrophils and 28% lymphocytes. Additional blood data were as follows: haemoglobin 11.9 g/dl, platelet count 170,000/µl and random blood sugar 120mg/dl. Serum electrolytes, LFT and KFT were normal. Chest x-ray and CT scan brain were unremarkable. Lumbar puncture yielded a clear cerebrospinal fluid (CSF) with a white blood cell count of 880/mm 3 (40% neutrophils and 60% lymphocytes), RBC 60/mm 3 , protein 65 mg/dl, glucose 16 mg/dl (simultaneous blood glucose level, 120 mg/dl) and negative results for India ink, acid fast and gram stains. An initial impression of bacterial meningitis and viral encephalitis was made and the patient put on intravenous acyclovir (30 mg/kg/day), ceftriaxone (100 mg/kg/day) and vancomycin (60 mg/kg/day). CSF culture on 5% sheep blood agar, after 24-hour incubation, grew small and showed white, smooth, translucent, moist colonies with subtle beta haemolysis. Gram stain showed pleomorphic short gram positive rods and coccobacilli, which exhibited a characteristic tumbling motility in hanging drop preparation. While a presumptive identification of L. monocytogenes was made, additional tests recommended for confirmation were put up. Acyclovir was withdrawn but vancomycin and ceftriaxone were continued. On the second and third day of hospitalization, the child continued to have intermittent spikes of fever, waxing and waning consciousness, irritability, excessive crying, shallow breathing and vomiting. She had extreme difficulty in swallowing. The child had also suffered several episodes of generalized seizures in the past 24 hours and developed bilateral lateral rectus palsies. Her pupils were dilated and sluggishly reacting to light. Phenobarbitone (3 mg/kg/day) and mannitol (1 g/kg infused over one hour as 20% sol) were added. On hospital day 4, isolate from CSF was confirmed as L. monocytogenes based on colony morphology, gram stain appearance, characteristic tumbling motility in hanging drop, umbrella motility in semisolid nutrient agar [Figure - 1], bile esculin hydrolysis, hippurate hydrolysis, CAMP positivity (with Staphylococcus aureus) and ability to grow at 4˚C. The isolate produced an acid /acid reaction in TSI without H 2 S and was positive for methyl red and voges proskauer but negative for nitrate reductase and urease. The organism utilized maltose and L-rhamnose but not D-xylose and mannitol. A final diagnosis of L. monocytogenes meningoencephalitis was made and the treatment changed to a combination of intravenous ampicillin (200 mg/kg/day) with amikacin (15 mg/kg/day). Within 48hrs of the change in treatment, the patient was afebrile, alert and cooperative. Her pupils were normal in size and briskly reacting to light. However, bilateral lateral rectus palsies persisted with left affected more than the right. After two weeks of treatment with ampicillin and amikacin, patient had almost fully recovered except for lateral rectus palsies that were still present. The child was playful and feeding but had profound sleep disturbances. Her blood and CSF counts had returned to near normal and repeat cultures were sterile. Patient was discharged and advised to continue ampicillin alone, for another week. She was HIV negative and her T cell function, nitroblue tetrazolium, serum complement and quantitative immunoglobulin levels were normal. T cell function was assessed by phytohaemagglutinin stimulation of lymphocyte ATP production. On her recent visit five months after the diagnosis; she was doing well other than her left lateral rectus palsy that had not resolved completely. Discussion L. monocytogenes may account for around 10% of community acquired meningitis, however, majority of these cases occur in newborns, pregnant women, the elderly and people with compromised immune function. [1],[9] Rarity of the infection beyond three months of age, in an immunocompetent child, makes clinical suspicion unlikely. The current case, a 20-month-old healthy immunocompetent child, was an unlikely candidate for listeriosis and as such, empirical treatment with ceftriaxone and vancomycin was started. Until, day 4 of hospitalization, when isolate from CSF was identified as L. monocytogenes, more than 72 hours on ceftriaxone and vancomycin had not caused any appreciable improvement in patient's condition. However, within 48 hours of substitution with ampicillin and amikacin, the child improved dramatically, was afebrile, alert and oriented. Empirical treatment with first line antibiotics like ceftriaxone and or vancomycin against community acquired meningitis can at times prove catastrophic if the causative agent is L. monocytogenes. Cephalosporins are inactive against Listeria and efficacy of vancomycin is variable as both successes and failures have been reported. [1],[2] Moreover, two weeks of treatment as recommended for community acquired meningitis due to other bacteria, can lead to relapses in Listeria meningitis, in which case, treatment for at least three weeks is more appropriate. [9] Intravenous administration of either ampicillin or penicillin, preferably in combination with an aminoglycoside, remain the drug of choice. [1],[2] L. monocytogenes may appear as pleomorphic short gram positive to gram variable bacilli resembling diphtheroids and as coccobacilli, diplococci or cocci resembling streptococci. Laboratory misidentification of L. monocytogenes as contaminant diphtheroids is not uncommon. As such, isolation of a small gram positive, catalase positive rod with a narrow zone of betahaemolysis isolated from blood or CSF should be used as a strong presumptive evidence for listeriosis. [1],[10] At times, even CSF examination (cytology and chemistry) can provide a strong lead. A lymphocytic pleocytosis with a low glucose concentration, as was in our case, can be highly suggestive of listerial meningitis in an appropriate setting. [9] Various foods implicated in causing listeriosis include contaminated coleslaw, ready to eat turkey, pate, pork products, hotdogs, delicatessen meats, butter, prepared salads, undercooked chicken and unpasteurised soft cheese and milk. [11] Our patient had no history of intake of any of these foods neither had she ever consumed refrigerated products. Nonetheless, the patient had consumed raw eggs continuously for about six weeks before she fell ill. Although eggs have been rarely incriminated, there are a few reports in literature. A documented case of fatal L. monocytogenes meningitis, reported in 1965, in a 39-year-old egg factory worker was conclusively traced to eggs. [12] In the current case, the probability of raw eggs serving the source of infection can not be completely ruled out. L. monocytogenes meningoencephalitis, is rare in immunocompetent post neonatal children. However, isolation of a gram positive rod from blood or CSF should never be regarded as a contaminant unless and until listeria has been ruled out. As treatment differs considerably from other causes of meningitis, proper and timely diagnosis can have a great impact on the final outcome. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10050f1.jpg] |
| |||||||||

{kind=link}