 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
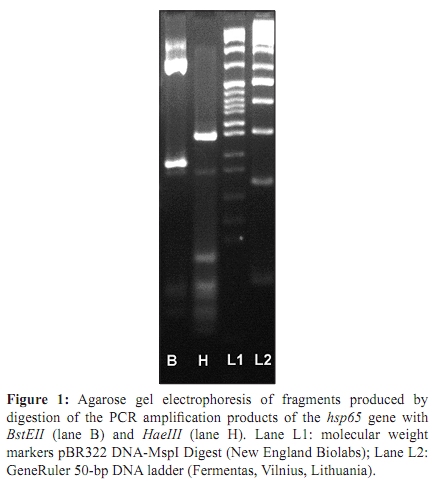
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 173-176 Case Report Mycobacterium arupense pulmonary infection: Antibiotic resistance and restriction fragment length polymorphism analysis *IK Neonakis, Z Gitti, F Kontos, S Baritaki, E Petinaki, M Baritaki, V Liakou, L Zerva, DA Spandidos Mycobacteriology Laboratory (IKN, ZG, MB, DAS), Department of Clinical Bacteriology, Parasitology, Zoonoses and Geographical Medicine, University Hospital of Heraklion, Heraklion, Greece. Correspondence Address: *Mycobacteriology Laboratory, Department of Clinical Bacteriology, Parasitology, Zoonoses and Geographical Medicine, University Hospital of Heraklion, Heraklion, Greece, ineonakis@gmail.com Date of Submission: 11-Jun-2009 Code Number: mb10052 PMID: 20404471 DOI: 10.4103/0255-0857.62502 Abstract Mycobacterium arupense is a novel mycobacterium species. It was first identified from clinical specimens in 2006 and since then there have been only two reports of its recovery from clinical samples. In the present case M. arupense was isolated from the sputum of a 62-year-old man with a malignant mass in his left kidney, who presented with a one-month history of recurrent fever, dyspnea and haemoptysis. M. arupense was identified with sequencing of hsp65 and 16S rRNA genes. In the present study, its biochemical profile along with its resistance status and hsp65 RFLP analysis is presented.Keywords: hsp65, Mycobacterium arupense, non-tuberculous mycobacteria Introduction In recent years, the application of molecular techniques has revolutionized the identification of mycobacteria. Sequencing analysis of 16S rRNA, 65 kDa heat shock protein (hsp65) and rpoB genes has been used to distinguish mycobacteria at the species level, [1] and several novel mycobacterial species have been described. Cloud et al. identified Mycobacterium arupense for the first time in June 2006, in the United States of America. [2] In the same year, there was a report from Japan by Masaki et al. and more recently from Taiwan by Tsai et al. [3],[4] The findings of these reports showed that isolates of M. arupense appeared to be clinically significant. [2],[3],[4] To our knowledge, the present study is the fourth worldwide to report on the recovery of M. arupense from clinical samples. Identification was achieved by sequencing of the 16S rRNA and hsp65 genes. The biochemical profile and resistance status of M. arupense along with restriction fragment length polymorphism (RFLP) analysis of its hsp65 gene are also presented. Case Report The patient was a 62-year-old man who presented to our hospital with a one-month history of recurrent fever, dyspnea and haemoptysis. His medical history included a large deficiency of the mitral valve and hypertension. A chest x-ray revealed extensive bilateral consolidation, predominantly in the middle lung fields, with marked bilateral pleural involvement, atelectasia due to pressure on the lung, and a small amount of pericardial fluid. The pleural collection was found to be an exudate without malignant cells. Computed tomography (CT) scanning revealed bronchoalveolar infiltration, in the presence of tumescent mediasthenal lymph nodes; a solid mass (11.7 x 11.8 x 9.6 cm) with calcifications on the left kidney, suggestive of malignancy. Baseline laboratory examinations revealed an elevated erythrocyte sedimentation rate (63 mm/h), a C-reactive protein concentration of 21.75 mg/dl, and a creatinin concentration of 4.1 mg/dl. Sputum samples were sent for common bacterial cultures; only one sputum sample was sent for mycobacterial culture. Immediately following sample collection, an empiric antibiotic regimen (levofloxacin, piperacillin/tazobactam and clarithromycin) was started. Clinically, the patient improved. The patient defervesced, and the haemoptysis and dyspnea subsided. The symptoms were not associated with the kidney mass and, at that point, the patient did not receive any treatment for the tumour. There were no further radiological findings concerning the mass lesion. The patient was discharged from the hospital after two weeks and programmed for further investigation of the kidney tumour in the future. All cultures for common bacteria were negative. The sample for mycobacterial culture was treated according to standard procedure. [5] A solid (Lowenstein-Jensen; LJ) and a liquid (MB/BacT/Alert 3D Automated System; bioMerieux, Durham, NC) culture were performed at 37 o C. Acid fast staining was negative. Growth was observed after five days of incubation in the liquid medium and after 10 days on LJ slants. The colonies were small, smooth and colourless. The Accuprobe assay (Gen-Probe, San Diego, CA) yielded negative results for Mycobacterium tuberculosis complex, Mycobacterium avium complex and Mycobacterium gordonae. The results of biochemical testing were: negative for nitrate reduction, arylsulfatase (three-day) and urease, and positive for â-galactosidase. This profile is in agreement with previous report.[2] No growth was observed on MacConkey agar without crystal violet at 37 o C and on LJ slants at 42 o C. The line probe GenoType CM and AS assays (Hain-Lifescience, Germany) showed non-species-specific banding patterns: 1, 2, 3 and 10 for CM and 1, 2, 3 and 12 for AM. Identification was achieved by sequencing the 16S rRNA and hsp65 genes. DNA from the isolate was extracted using a guanidinium thiocyanate lysis buffer as previously described. [6] A small number of mycobacterial colonies were suspended in 600 ìl of lysis buffer (Guanidinium thiocyanate 4M, 0.5% N-lauryl sarcosine, 1 mM dithiothreitol, 25 mM sodium citrate and 50 ìg of glycogen) and incubated overnight at room temperature. A total of 600 ìl of ice-cold (-20o C) isopropyl alcohol was then added. After 1.5 hours the sample was centrifuged for 10 minutes (16,600 g, 4 oC). Isopropyl alcohol was removed and the pellet was washed with 70% ethanol. The dried pellet was dissolved in 50 ìl of DNAse and Rnase-free double-distilled sterile water. A 1340-bp product containing nearly the full length of the 16S rRNA gene was amplified in an automated DNA sequencer (3730 DNA analyzer, Applied Biosystems) using the Big Dye terminator sequencing kit (Applied Biosystems, Carlsbad, California, USA) and the F16S and R16S primers, as previously described. [7] The sequence was aligned with the sequences in the GenBank database ( www.ncbi.nlm.nih.gov ), showing 100% similarity (1340/1340 identities) with the 16SrRNA gene of the M. arupense strain AR30097 (DQ157760), 99.9% similarity (1339/1340) with the M. arupense strain CST7052 (AB239926) and 99.8% similarity (1337/1340) with the M. arupense strain CST0506 (AB239927). Moreover, a 439-bp fragment of the hsp65 gene was amplified using the protocol and the primers Tb11 and TB12, as previously described. [8] The sequence showed 100% similarity (386/386) with the hsp65 sequence of M. arupense isolate FI-05354 and 99% similarity (419/422 identities) with several M. arupense strains, such as AR30097 (DQ168662), CST7052 (AB239922) and CST0506 (AB239924). The 16S rRNA and hsp65 gene sequences have been deposited in GenBank with the accession numbers FJ403044 and FJ263631, respectively. The PCR product of hsp65 was further used for RFLP analysis. PCR product (12 ìL) was digested with HaeIII (New England Biolabs, Ipswich, MA, USA) and BsteII (New England Biolabs), and the restriction mixture was run on 3.5% metaphor agarose gel (Cambrex Bioscience, Rockland, ME, USA) at 100 V. BstEII digestion produced two fragments of 325 and 115 bp, and HaeIII digestion produced four fragments of 145, 60, 50 and 40 bp [Figure - 1]. Susceptibility testing of the isolate was performed using the E-test method (AB Biodisk, Solna, Sweden) according to the manufacturer's instructions. The antibiotics tested and the minimum inhibitory concentrations obtained (in parenthesis) were: amikacin (1 ìg/ml), ciprofloxacin (4 ìg/ml), clarithromycin (0.25 ìg/ml), ethambutol (0.032 ìg/ml), ethionamid (0.25 ìg/ml), linezolid (8 ìg/ml), levofloxacin (4 ìg/ml), rifampicin (0.5 ìg/ml), streptomycin (1 ìg/ml) and trimethoprim-sulfomethoxazol (>32 ìg/ml). The results were evaluated as previously described.[4],[9],[10],[11] According to available breakpoints, susceptibility was found for amikacin, clarithromycin, ethambutol, ethionamid, linezolid and streptomycin whereas, resistance was found for ciprofloxacin, levofloxacin and trimethoprim-sulfomethoxazol. Discussion Mycobacterium arupense is a novel mycobacterium species. The present study is the first report from Greece and among the first worldwide to document its recovery from clinical samples. In the present study the biochemical profile of Mycobacterium arupense, its resistance status and its hsp65 RFLP banding pattern were also presented. M. arupense was first identified by Cloud et al. in several clinical specimens, mainly sputa and bronchial wash specimens. [2] Moreover, it was isolated from sterile sites (lymph node, lung biopsy, pleural fluid, surgical tissue and urine), indicating that M. arupense can be the cause of human disease. [2] However, the authors noted that additional information was needed to gain insight into the clinical significance of this organism. In the report by Masaki et al., M. arupense was isolated in two specimens from Japanese men: (a) sputum from a 60-year-old patient with an abnormal shadow by indirect x-ray and (b) pus from a 68-year-old patient with purulent tendovaginitis. [3] The latter patient recovered after the operation and the antimicrobial treatment administered, leading the authors to suggest that the organism was clinically relevant. [3] Tsai et al. (2008) described the case of a 54-year-old woman with swelling and pain of her left middle finger and a tender nodule in the middle of her palm. [4] Six months earlier, she had been involved in a motorcycle traffic accident and noted a mildly tender nodule on her left palm one month later. A specimen was obtained by incision and the culture grew a mycobacterium species that was later identified as M. arupense by sequencing. The patient received a multi-drug treatment for six months, and her condition improved. [4] The principal issue concerning non-tuberculous mycobacteria (NTM) is whether the presence of an NTM is merely colonization or the cause of disease. Many physicians make this determination according to the American Thoracic Society (ATS) criteria, [12] which require three positive cultures from sputum samples to characterize an NTM as the cause of the disease. However, it should be noted that in everyday hospital practice the documentation called for by the ATS criteria is hard to achieve. Patients with pulmonary infections are admitted to hospitals, where routine pulmonary samples are taken for common bacterial cultures. In certain cases only one sample is sent for mycobacterial culture. Usually, immediately after sample collection, an empiric antibiotic treatment is administered. This happened with our patient. In most cases the empiric treatment includes quinolones and/or MLS (Macrolides, Lincosamides, Synergystins), which are usually effective against the majority of NTMs. Thus, even if cultures for common bacteria are negative and result in additional samples being sent for mycobacterial cultures, these cultures are also likely be negative. It should be noted that although physicians include mycobacteriosis in their differential diagnosis list when tending to patients with a recurrent fever, and despite the fact that patients suffering from mycobacterial disease usually are not acutely ill, physicians usually do not apply the proper protocol for sample collection. Such a protocol should be: one sample on arrival, one sample the following morning and a third sample when the second specimen is delivered to the laboratory. Based on the ATS criteria, the case presented in this study should be characterized as one of colonization with only one isolation of the strain. However, the fact that no other bacterium (either common or mycobacterium) was isolated and the fact that the patient improved clinically with the administered antibiotic therapy suggest that the possibility of infection due to M. arupense cannot be ruled out. Nevertheless, M. arupense is a new mycobacterium and further data are required for its pathogenic potential to be assessed. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10052f1.jpg] |
| |||||||||
{kind=link}