 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
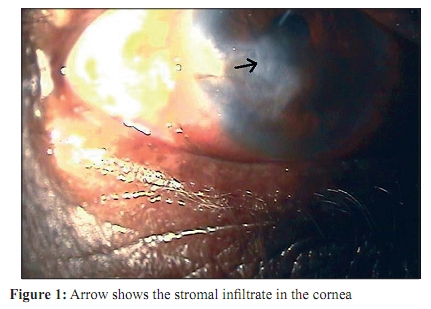
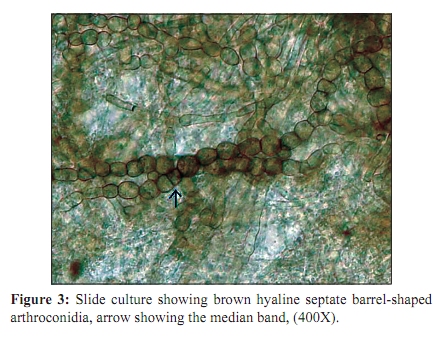
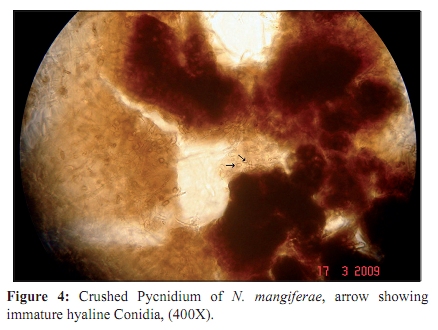
Indian Journal of Medical Microbiology, Vol. 28, No. 2, April-June, 2010, pp. 178-181 Case Report Nattrassia mangiferae causing fungal keratitis *AJ Kindo, S Anita, S Kalpana Departments of Microbiology (AJK, SA), Ophthalmology (SK), Sri Ramachandra Medical College and Research Institute, Porur, Chennai - 600 116, India Correspondence Address: *Department of Microbiology, Sri Ramachandra Medical College and Research Institute, Porur, Chennai - 600 116, India, anupmalakra@yahoo.com Date of Submission: 03-Apr-2009 Code Number: mb10054 PMID: 20404473 DOI: 10.4103/0255-0857.62504 Abstract We report a case of fungal keratitis caused by the coelomycetous fungus Nattrassia mangiferae in a 70 year old gentleman, agriculturist by occupation, with a history of injury to his right eye. The scraping showed narrow septate fungal hyphae on a KOH mount, isolation of a fast growing black mould, which demonstrated hyphae and arthroconidia of varying widths typical of the Scytalidium synanamorph (S. dimidiatum). The formation of the pycnidia, which at maturity, expressed conidia. The patient was started on topical itraconazole one hourly and topical atropine thrice a day. The patient was lost to follow up hence we are not able to comment on the final outcome of the patient.Keywords: Coelomycetes, fungal keratitis, Nattrassia mangiferae Introduction Coelomycetes fungi appear to be increasing in incidence in human disease. They are frequently acquired through some type of traumatic implantation and are of particular concern in patients being maintained on long term immunosuppressive therapy. [1] Although the recovery of these fungi in the laboratory is not particularly difficult, identification of some species remains laborious due to poorly defined, difficult to assess criteria and atypical characteristics displayed under artificial growth conditions. The coelomycete N. mangiferae (synanamorph Scytalidium dimidiatum) is a filamentous fungus, which was first described in 1916 as Dothiorella mangiferae[2] until recently, it was reclassified as Hendersonula toruloidea Nattrass.[3],[4] In the latest revision of the Hendersonula, it was reclassified in its own genus based on its pycnidial stage. [5] In addition, the Scytalidium synanamorph was proposed for its arthroconidial stage because pycnidia might be difficult to detect or could be absent, as is the case of slow growing isolates. [6] N. mangiferae may sometimes be misdiagnosed as Scytalidium lignicola. However, Scytalidium lignicola is distinguished by the hyaline, uniformly narrow, usually unbranched, fertile hyphae arising as lateral branches from the vegetative mycelium. However, in Scytalidium dimidiatum the arthroconidia are more variable in width and color.[7] Case Report A 70-year old gentleman, agriculturist by occupation, came to Ophthalmology Out Patient Department with history of injury to his right eye caused by the spokes of an umbrella three months ago. He was not a known diabetic or hypertensive; there was no other significant history. He had consulted an ophthalmologist in another hospital and was diagnosed to have a fungal corneal ulcer. He was started on topical natamycin, atropine and oral pain killers. There was no improvement in his condition, which made him come to our OPD. Examination findings of his right eye were as follows: Best corrected visual acuity: 6/60 The lid was edematous. There was circumcorneal congestion. Cornea had 5 mm x 3 mm stromal infiltrate in the inferotemporal quadrant involving the visual axis [Figure - 1]. The surrounding cornea was hazy with microcystic epithelial edema and stromal edema; the anterior chamber had dense reaction with 3+ flare, cells and 2 mm hypopyon. The fundus could not be visualized as the media was hazy. Corneal scraping was sent to the Microbiology Department to find out the etiological agent. The Gram stain showed plenty of pus cells and the, KOH wet mount showed plenty of fungal filaments. The specimen was inoculated in SDA plates (C shaped inoculation) in the OPD by the ophthalmologist. The colonies grew rapidly within 4-7 days. The isolate was further subcultured in SDA tubes and incubated at 37 o C and 25 o C. The fungal growth was whitish grey, becoming olivaceous grey to black, overlaid with aerial strands of greyish black mycelia. [Figure - 2]. The reverse was initially buff, but darkened to a greyish black. The slide culture of the isolate put in oat meal agar demonstrated septate, branched, subhyaline to dark brown hyphae, fragmented to form cylindrical or barrel-shaped, subhyaline to dark brown, non-septate or one septate arthroconidia [Figure - 3]. Conidia on maturity (requiring several more weeks), developed one or two septa and a brown median band. Pycnidia developed within two to three weeks. To promote the development of the pycnidial stage, the isolate was grown on pieces of banana peel in water agar. [7] Five-millimeter-wide strips of peel, sterilized by autoclaving in glass petri dishes with 5 ml of water at 121 o C for 15 minutes were inoculated with fragments of mycelium and were incubated in moist chambers at room temperature in an ambient atmosphere. The pycnidial conidia were hyaline and oval in shape [Figure - 4]. The fungus was identified as N. mangiferae / S. dimidiatum by its colonial and microscopic features. Nattrassia mangiferae, although very slow to form, is a mature, versicoloured (darkened middle cell and pale end cells) arthroconida, easily recognized by its distinctive Scytalidium lignicola and Scytalidium hyalinum synanamorphs [Figure - 3]. The patient was started on topical itraconazole hourly and topical atropine tds. Discussion Coelomycetes incite a variety of clinical entities. The method of acquisition is frequently by implantation of the fungus from plant / woody material or the soil through abrasions, lacerations, puncture wounds or other traumas into the cutaneous / subcutaneous tissue, rather than by inhalation of the conidia. Initial presentations in this setting are often superficial or ocular, with subsequent progression to invasive, subcutaneous disease. [1] Reports have included facial lesions, mycetoma, subcutaneous abscesses, fungemia and endophthalmitis. [4],[7] Although human skin and nail infections due to this fungus are well documented, [8] Nattrassia mangiferae causing keratitis is relatively rare. Immunosuppression is typically the underlying condition that predisposes a patient to develop opportunistic infection. Other than the age factor the patient described here had no obvious underlying disease. Corneal phaeohyphomycosis is caused by Lasiodiplodia theobromae, Curvularia geniculata, Curvularia lunata and Exophiala jeanselmei and have been reported. [9] As many pathogenic or saprophytic fungi can also produce arthroconidia in culture, differentiation between N. mangiferae and arthroconidial fungi should be considered. Coelomycetes fungi usually exhibit a moderate-to-rapid growth rate on a variety of media and are not particularly difficult to recover from specimens. The problem lies in promoting diagnostic reproductive structures necessary for characterization of the isolates. Not only is a considerable amount of time required, particularly for the pycnidial species (it took 2 months in our strain), but it is also necessary to utilize a medium in which these pycnidia will develop. We used sterilized banana peel on water agar, which helped in producing conidomata, more representative in nature. Another medium frequently cited as useful in coelomycetes is oatmeal agar. [1] These organisms are frequently very refractory to antifungal therapy and require long-term dosing regimens for eradication. [10] The patient described here did not respond to natamycin topical application and after identifying the fungus responsible for the infection, was changed to hourly itraconazole eye drops. After the final identification of the fungus, the change of eye drops to amphotericin B was being considered, but unfortunately the patient did not turn up for follow up and hence we were not able to assess the response of the treatment in this patient. Conclusion Fungal keratitis is responsible for the significant burden of the blinding disease in the developing world. Current treatment methods fail to preserve or restore vision after fungal keratitis. Scytalidium spp fungal organisms can cause an indolent keratitis, intensive oral and topical antifungal therapy is required for eradicating the infection. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10054f2.jpg] [mb10054f1.jpg] [mb10054f4.jpg] [mb10054f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}