 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 221-226 Original Article KatG protein: A novel marker for differential diagnosis of Myobacterium avium complex infection K Gupta1, I Verma2, G Khuller2, R Mahajan3 1 Department of Biochemistry, PGIMER, Chandigarh-160 012; ( Presently Department of Biochemistry, AIMSR, Bhatinda-151 109), India Material and Methods:Initially, a specific protein band of ~80-85 kDa was recognised by differential immunoblotting; which was subjected to anion exchange column chromatography for purification of proteins. After fractionisation using SDS-PAGE and electroelution, blast search was carried out. Further immunoreactivity studies were done with M. avium and Mtb infected mice sera. Clinical utilisation of separated protein was evaluated by conducting indirect ELISA with serum samples from mycobacterial infected patients. Results: A specific 81.6 kDa protein, shown to be catalase-peroxidase protein (KatG) by blast search was separated. Immunoreactivity studies of purified KatG proteins with mice sera confirmed it to be specific for M. avium infection. Indirect ELISA with patient samples further confirmed it to be M. avium infection specific. Conclusion: KatG protein is specifically recognised by MAC patients and can be used as a marker for simple and rapid ELISA based tests for differential diagnosis of M. avium infection. Keywords: Differential diagnosis, enzyme linked immunosorbent assay, mycobacterium avium infection, secretory proteins Introduction Disease due to the Mycobacterium avium complex (MAC) is one of the most important opportunistic pulmonary infections. [1] Disseminated MAC infection is a severe complication of advanced human immunodeficiency virus (HIV) disease. [2] Incidence of MAC infection is increasing even in immunocompetent pulmonary disease patients. [3] Studies have reported that pulmonary diseases caused by MAC in non-HIV infected persons are as common as pulmonary tuberculosis in many areas. [4] Early differential diagnosis of Mycobacterium avium in clinical samples is becoming increasingly important because of growing frequency of MAC infection in immunocompetent patients, [3] impeding availability of new drugs, [5] clinical features resembling tuberculosis and difficult chemotherapy as compared to Mycobacterium tuberculosis[1] and poor prognosis of disseminated MAC disease. [6] Till date, several diagnostic methods and techniques for differential diagnosis of M. avium infection; like biochemical tests based diagnostic procedures, [7] 125 I-labeled cDNA probe assay, [8] phenotypic identification of culture by hybridisation protection assay, [9] nucleic acid based approaches [10] and ESAT-6 polymerase chain reaction (PCR) primers [11] have been reported. These methods have their own limitations; they either lack sensitivity, or are time consuming, or carry the risk of radioactivity or are so complex to be performed routinely. So the development of simple and rapid diagnostic method for differential diagnosis of M. avium infection is the need of the hour. Serodiagnostic techniques, based upon the recognition of species specific proteins secreted by actively growing myobacterial bacilli in the culture filtrate have been advocated to be simple, easy, cost-effective and rapid methods. [12] In addition, this is a highly sensitive technique; capable of detecting mycobacterial antigens at a concentration of 10 -9 /ml. [13] Taking care of these findings, the present study was designed to identify, isolate and purify Mycobacterium avium specific secretory proteins and to evaluate the role of these proteins in the diagnosis of M. avium infection. Material and Methods This is an ethically designed study, fully approved by Institutional Animal Ethical Committee and Institutional Human Ethical Committee. Study population
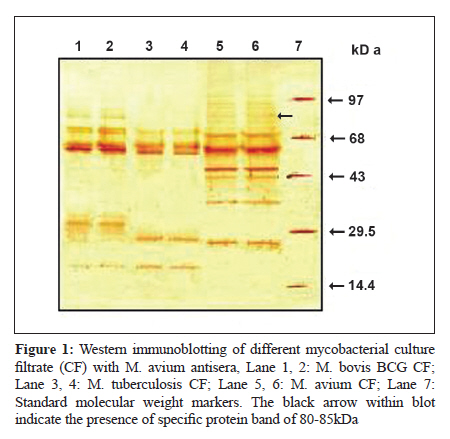
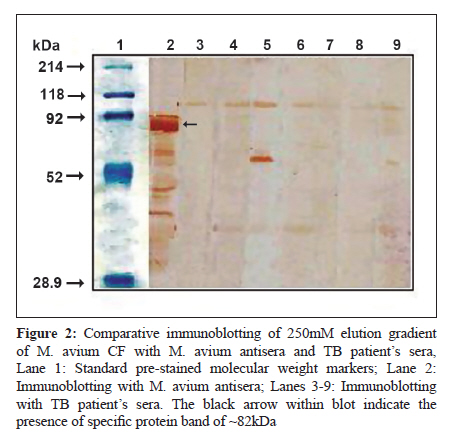
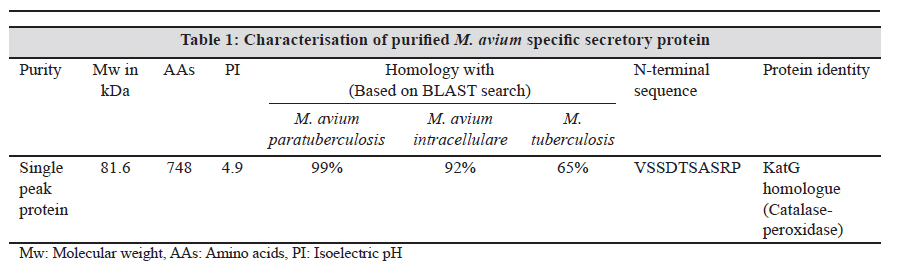
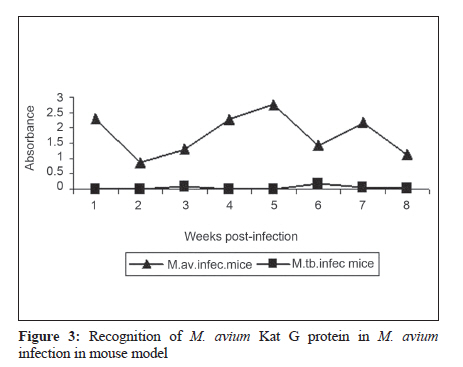
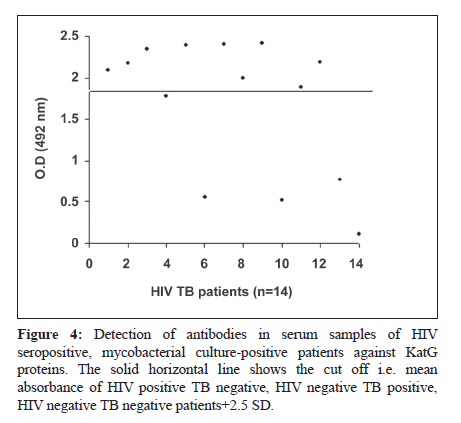
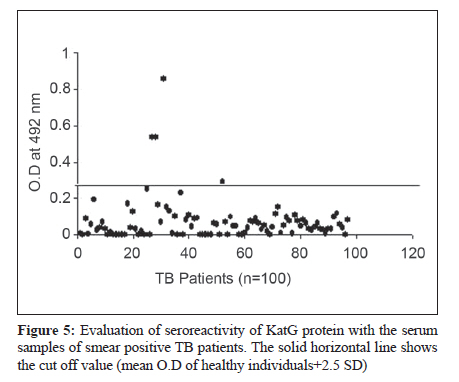
For detection of antibodies present against M. avium specific proteins, 1 ml of blood was withdrawn from all participants, after taking informed written consent. Mycobacterial culture Mycobacterium avium subsp. avium 1723 (NCTC 8551, originally isolated from pig liver) was obtained from Microbial Type Culture Collection, Institute of Microbial Technology, Chandigarh, India; while Mycobacterium tuberculosis H 37 Rv and Mycobacterium bovis BCG were obtained from National Collection of Type Cultures, London, UK. These strains were maintained on Lowenstein Jensen′s Medium and Modified Youman′s Medium [14] in the laboratory and subsequently used in the study. Animals Forty BALB/c mice of either sex (20-25 gm body weight, 4-5 weeks) were obtained from Central Animal House, PGIMER, Chandigarh, India. Animals were housed in cages kept in negative pressure regulated animal isolators and fed on standard pellet diet (Hindustan Lever Ltd., Mumbai) and water ad libitum. Infection of animals and isolation of antisera In order to obtain M. avium and other mycobacterial antisera for comparative ELISA and western immunoblot studies, 10 Balb/c mice per group were infected with 1x10 6 bacilli of different mycobacterial species by intravenous route and categorised as follows: Group 1 - Control group, mice injected with normal saline Group 2 - Mice infected with M. avium Group 3 - Mice infected with M. tuberculosis Group 4 - Mice challenged with M. bovis BCG Blood was collected on 2 nd , 4 th , 6 th , 8 th , 10 th and 12 th weeks post infection, sera was separated and stored at -20 0 C till further use. Isolation of short-term culture filtrate (STCF) and identification of M. avium specific proteins by 1-D SDS-PAGE M. avium, M. tuberculosis H 37 Rv, M. bovis BCG were grown on the modified liquid synthetic Youman′s medium as a stationary pellicle culture at 37 0 C for four to five weeks. Sterilisation was done by passing the culture filtrate (CF) through 0.22 ΅m millipore assembly. CF proteins were initially concentrated and washed with PBS on Tangential flow system (Millipore Inc; Bedford, USA) and finally through (100 X) Amicon YM-3 ultrafiltration assembly (Millipore Inc; Bedford, USA). The protein content of isolated culture filtrate was determined [15] and the protein profiles of different mycobacterial culture filtrates were analysed by 1-D Sodium dodesyl sulphate- Polyacrylamide gel electrophoresis (SDS-PAGE) (Hoefer SE 600, Amersham Pharmacia, Biotec Inc, San Francisco, USA) followed by silver staining. Aliquots of culture filtrate proteins were finally stored at -20oC till further use. Identification and confirmation of M. avium specific secretory protein(s) by 1-D western immunoblotting and their purification Different mycobacterial culture filtrates separated on 12% SDS-PAGE were transferred on nitrocellulose paper (NCP) using semi-dry electroblotting apparatus (Bio-Rad; USA). Confirmation of complete transfer was done by pre-stained molecular weight marker followed by incubation of the membrane with 3% BSA in PBS (pH 7.4), overnight, at 4oC. After the subsequent washes with PBS containing tween-20 (2%), the membranes were incubated with different mycobacterial antisera (M. avium antisera, M. tuberculosis H 37 Rv antisera, M. bovis BCG antisera and pre-immune sera) diluted (1:100) in PBS containing 1% BSA for 2hrs at room temperature on orbital shaker with gentle shaking. After six washes the membrane was again incubated with antimouse IgG-HRP conjugate diluted in PBS containing 1% BSA (1:2000) for two hours at room temperature. NCP was then washed six times to remove unbound conjugate and finally developed with diaminobenzedine (DAB) in PBS-H 2 O 2 substrate buffer. After development of blot, reaction was stopped immediately by washing NCP with distilled water. The M. avium specific secretory proteins identified and confirmed on the basis of 1-D SDS-PAGE and western immunoblotting were purified using combination of anion-exchange column chromatography and electroelution. Confirmation of specificity of purified M. avium Specific protein Purified M. avium specific proteins were subjected to western immunoblotting with M. avium antisera, M. tuberculosis antisera, M. bovis BCG antisera, TB patient′s sera, and healthy individual′s sera to check whether the proteins are recognised in the mycobacterial infections other than M. avium. Purified M. avium specific proteins were transferred to NCP after blocking with 3% BSA and subsequent washings; the membrane was incubated with the appropriate dilution of various antisera (1:100). Antimouse/antihuman HRP conjugate (1:2000) was used and the reaction was developed with DAB-H 2 O 2 substrate buffer in PBS (pH 7.4). Characterisation of M. avium specific secretory proteins M. avium specific secretory proteins selected on the basis of specificity in the diagnosis of M. avium infection were subjected to LC-MS-MS for the determination of their isoelectric pH (PI), total amino acid content, theoretical molecular mass and sequence of internal peptide fragments. This characterisation was done at Dr. J.T. Belisle′s laboratory, Department of Microbiology, Colorado State University, Fort Collins, Colorado, USA. LC-MS-MS (Bruker Bremen, USA) was performed by in-gel proteolytic digestion with trypsin. Peptides were eluted from the acrylamide and separated by C18 capillary reverse phase chromatography. [16] Evaluation of diagnostic potential of M. avium specific proteins for identification of M. avium disease To check the significance of M. avium specific proteins in the diagnosis of M. avium infection in a clinical set-up, M. avium infected patients were selected from HIV positive population on the basis of culture positivity on the culture media and by battery of biochemical tests. The M. avium specific secretory proteins were subjected to indirect ELISA with 1:100 dilution of sera of HIV -ve TB +ve patients, HIV +ve TB +ve patients, HIV +ve TB -ve patients, M. avium antisera, M. tuberculosis antisera and healthy individual′s sera to check their specificity for the diagnosis of M. avium infection. Results The protein content of the culture filtrate obtained after harvesting the mid log phase of different mycobacterial species was 15 ± 3 mg/ml. The culture filtrate proteins resolved on 12% denaturing gel showed the presence of protein bands ranging from the molecular weight of 6kDa to 97kDa on SDS-PAGE, but in M. avium CF the protein band in the regions of 80-85kDa seemed to be specifically present and absent from rest of mycobacterial species. The immunoblotting of M. avium, M. tuberculosis H 37 Rv and M. bovis BCG CF proteins with M. avium antisera also indicated the presence of number of common protein bands in all the mycobacterial species. However, M. avium culture filtrate immunoblotted with M. avium antisera showed some specific protein bands of 80-85kDa [Figure - 1] that were not evident in others [Figure - 1]. Anion exchange column chromatography resulted in the elution of an immunodominant protein of ~82kDa in 250 mM elution gradient. Comparative immunoblotting of ~82kDa protein of 250mM elution gradient with M. avium antisera, M. tuberculosis antisera (taken as positive and negative control respectively) and TB patient′s sera showed that these proteins has reactivity only with M. avium antisera, while with TB patient′s sera and M. tuberculosis antisera, no recognition was detectable [Figure - 2] depicting the specificity of these proteins for M. avium infection. On LC-MS-MS ~82 kDa protein was found to be highly pure protein demonstrating a single peak in the mass-spectra. The protein was observed to be KatG homologue (Catalase-Peroxidase) of molecular weight 81.6 kDa with 748 amino acid and PI of 4.9. With blast search, it was found to be 99% homologous with the KatG protein of M. avium paratuberculosis and 92% with M. avium intracellulare and other members of MAC, while with M. tuberculosis the protein homology was 65% starting at 41 st amino acid. The N-terminal sequence of the protein was found to be different from M. tuberculosis, and demonstrated 100% homology with M. avium 104, the clinical isolate of M. avium with highest disease prevalence in HIV positive patients [Table - 1]. Immunoreactivity studies of purified KatG protein with M. avium and Mtb infected mice sera demonstrated the presence of KatG antibodies only in M. avium antisera [Figure - 3] and confirmed the specificity of M. avium KatG protein for M. avium infection. Significance of purified M. avium KatG protein in the diagnosis of MAC in clinical set-up was confirmed by indirect ELISA with the patients with MAC bacteraemia, selected from HIV +ve population with disseminated mycobacterial disease on the basis of blood culture by lysis centrifugation method, followed by a battery of biochemical tests. Out of 54 blood samples of HIV patients with disseminated mycobacterial infection, 14 samples were mycobacterial culture positive and of these 14 samples, 10 were MAC and four were Mtb positive on the basis of biochemical tests. When purified M. avium KatG protein was subjected to indirect ELISA with the serum samples (1:100 dilutions) of these 14 patients, nine out of 10 MAC positive patients had antibodies to recognize the protein giving a percent recognition of 90%. [Figure - 4] Four samples that were positive for Mtb did not recognize KatG, confirming that this protein is specific to M. avium infection. Further, M. avium KatG protein based ELISA in the serum samples from 100 pulmonary TB patients demonstrated that 96/100 patients showed no reactivity, thus confirming the specificity of M. avium KatG based serodiagnostic assay. [Figure - 5] Also, the absence of anti-KatG antibodies in healthy BCG vaccinated individuals further confirmed the recognition of this protein only during active disseminated MAC disease and showed that it is not affected by prior BCG vaccination/ exposure to environmental mycobacteria. Kinetic-expression studies performed by immunoblotting M. avium CF with M. avium antisera collected at weeks 2, 4, 6, 8, 10 and 12 after experimental M. avium infection in mouse model showed that KatG protein was recognized as early as from week 2 post infection, although the expression of antibodies in week 2 to 4 post infection sera was relatively low. From weeks 6 to 10, post-infection, the expression was greatly enhanced. Discussion The conventional blood culture and biochemical test for differential diagnosis of M. avium infection are time consuming. Isolation of MAC by conventional mycobacterial culture on tubed solid medium generally takes three to four weeks. [17] Identification by biochemical test is complex and also time consuming process depending upon the culture growth that may take 2-4 weeks, because of long generation time of mycobacteria. [18] This latent period of three to four weeks can lead to delay of therapy and worsening of symptoms. As the organisms are commonly found in the environment so contamination of the culture material or the transient infection may also occur. Bone-marrow specimen based test for detection of M.avium infection had proved to be more invasive and provided no advantage over blood culture based tests. [19] As stated earlier, other methods have their own limitations; they either lack sensitivity, or carry the risk of radioactivity or are too complex to be performed routinely. Early diagnosis and treatment may prolong survival in patients with acquired immune defieciency syndrome and MAC infection. [20] The diagnostic criteria currently followed by Revised National Tuberculosis Control Programme in accordance with American Thoracic Society (ATS) guidelines for M. tuberculosis and M. avium respectively are based on the radiological findings, sputum smear examination and response to antituberculous therapy especially in endemic countries. [21] However, low sensitivity of smear microscopy especially in children, HIV infected TB patients, and extra pulmonary cases are the compelling reason to explore the possibility of developing new diagnostic tests for the differentiation of disease caused by M. avium and M. tuberculosis. Since proteins secreted by mycobacteria has been thought as the primary target during initial phase of the infection, therefore development of sensitive and specific immunodiagnostic procedures based on specific secretory proteins for the rapid detection of M. avium infections would greatly facilitate clinical management of active disease. The diagnosis of M. avium disease on the basis of distinct and specific antigens would be sensitive and specific, as only M. avium infected patient′s sera will recognize the species-specific proteins. KatG (a 81.6kDa, single peak secretory protein) based ELISA has an overall sensitivity of 90% and specificity of 96% in diagnosing MAC infection. Further, this protein is recognised as early as week 2, post-infection. Moreover, this test can also be applied to HIV positive/AIDS patients, which do not respond to T-cell based assays due to very low CD4 + T-cell counts. This data clearly demonstrates that the M. avium KatG protein is able to differentially diagnose disseminated MAC disease in HIV infected population at an early stage and the results obtained with antibody-based easy and rapid ELISA test correlate with conventional time-consuming blood culture and biochemical tests. To conclude, this study clearly indicates that the development of M. avium KatG based diagnostic ELISA could be of great help to clinicians in the timely diagnosis and treatment of disseminated MAC disease in HIV patients. Acknowledgment We thank the faculty members of TB and Chest Diseases Hospital, Patiala who provided clinical assistance for the study. We also thank Dr. Suman Lal and Dr. Karen Dobos, Colorado State University, Colorado, USA for the LC/MS analysis of KatG protein. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10068f1.jpg] [mb10068f2.jpg] [mb10068f5.jpg] [mb10068t1.jpg] [mb10068f4.jpg] [mb10068f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}