 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
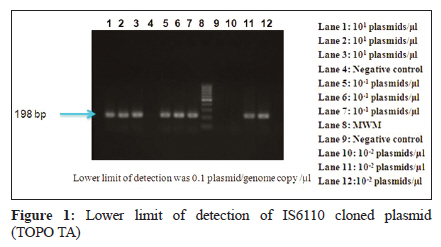
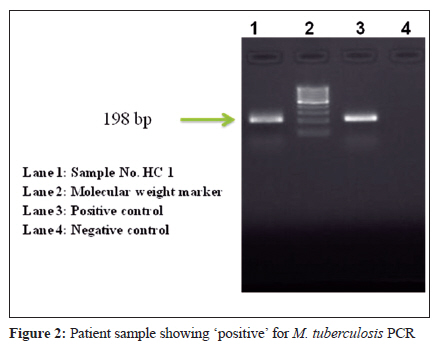
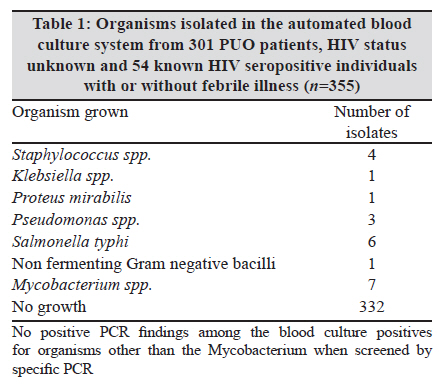
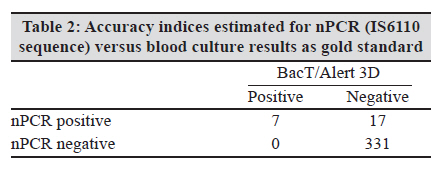
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 227-232 Original Article Evaluation of a nested PCR targeting IS6110 of Mycobacterium tuberculosis for detection of the organism in the leukocyte fraction of blood samples B Nandagopal1, S Sankar1, K Lingesan1, KC Appu1, G Sridharan1, AK Gopinathan2 1 Sri Narayani Hospital & Research Centre, Thirumalaikodi, Sripuram, Vellore - 632 055, India Keywords: Buffy coat, Mycobacterium tuberculosis, nested PCR, IS6110, rural Introduction In India, the annual incidence of tuberculosis per 100,000 population was reported to be 283 in 2007. [1] The prevalence of HIV seropositives among tuberculosis patients was 5.3% in India. [1] The burden of tuberculosis is further enhanced because of the HIV epidemic which predisposes to infection with M. tuberculosis and mycobacteria other than M. tuberculosis (MOTT). [2] In India, the mortality rate has increased by 22% over the previous years. [3] This problem has to be taken serious note of while devising strategy for tuberculosis control. Sputum smear microscopy with Ziehl-Neelsen staining is the most widely used rapid method in most laboratories for diagnosing tuberculosis under the Revised National Tuberculosis Control Programme (RNTCP). Raizada et al. [4] have pointed out that among HIV infected individuals smear examination is less successful than in HIV uninfected individuals with pulmonary tuberculosis, a situation seen also in extra-pulmonary tuberculosis . This indicates a need for extensive screening for tuberculosis in HIV positive patients. However, the Ziehl-Neelsen smear technique suffers from several limitations such as low sensitivity and specificity, especially in extra-pulmonary manifestations. Culture of M. tuberculosis in LJ medium, the gold standard for laboratory diagnosis, though sensitive, is laborious and takes four to eight weeks and should be followed by identification tests such as niacin test. Pulmonary specimens such as sputum are used after extensive processing steps. Fandinho et al. [5] had, earlier, investigated a lysis centrifugation method to detect mycobacteraemia. They reported a mean detection time of 42 days. Subsequently, Ramachandran et al. [6] examined the use of radiometric Bactec method to detect mycobacteraemia in HIV infection and reported the time taken for identification ranged from 22-43 days. Even such methods do not enhance the speed of diagnosis sufficiently, which ultimately delays the treatment leading to mortality. In India, many individuals present with undifferentiated fever which is categorised as PUO pending specific investigation for tuberculosis. [7] This problem has to be addressed by improving the comprehensive diagnosis of infectious aetiology of PUO in India. Insertion element, IS6110, is an ideal target for PCR as it is estimated that individual bacterium has one to 10 copies of this insert. [8] We report here the evaluation of the nPCR in buffy coat (WBC) of the blood sample collected from patients with PUO and known HIV positive individuals. We chose buffy coat as the specimen of choice as M. tuberculosis is reported to infect monocytes and can be detected from peripheral blood. The results of the nPCR were compared to an automated commercial blood culture system. Materials and Methods This study was approved by the Institutional Review Board (IRB) of our institution. A total of 355 samples were collected from patients during the period of Nov 2008 to Jun 2009. The study described here is cross-sectional in nature, the clinical sample i.e. blood was collected at the first time of contact with the patient by the study physician. A detailed questionnaire and consent form was obtained for each patient. In all, blood samples were collected from patients in a tertiary care multi-specialty hospital situated in a rural area of Vellore district. Specimens Among the patients recruited for the study, the HIV status of 301 patients with pyrexia of unknown origin (PUO) was unknown, whereas, 54 patients additionally recruited were known to be seropositive for HIV. The HIV positive individuals were recruited from Community Care Centre (CCC) of the hospital where these individuals were admitted for illness episodes during anti-retroviral therapy initiated at the ART centre of Government Vellore Medical College Hospital, Adukambarai, Vellore, situated 5 km away from the study centre. The 301 patients with PUO recruited for the prospective study included those with a history of an acute/chronic undifferentiated febrile illness (temperature of 101°F) of 5 to 15 days or more or who were admitted to the medical wards when the patient′s condition required hospitalisation. The patient′s consent was obtained for all individuals. Fever was recorded for every patient and the temperature ranged from 99 to 106°F, the duration of fever was between 2 and 365 days. The exclusion criteria primarily were causes of immunosuppression other than HIV infection, haematological malignancy, autoimmune disorders, and immunosuppressive therapy. We also excluded those with obvious focus of acute infection such as urinary tract infections, lower respiratory tract infections, bacterial meningitis and suppurative abscesses. Sample collection Venous blood samples (15mL) were collected; 5mL for routine blood culture and 5mL for M. tuberculosis culture. The other 5 mL was collected in a sterile falcon tube containing EDTA for buffy coat preparation. Blood culture was done in a completely automated blood culture system, BacT/Alert 3D® (Biomιrieux, NC, USA) according to the manufacturer′s instructions. The blood culture results were communicated to the treating physicians in real time. Buffy coat preparation and DNA extraction Buffy coat was prepared from the third fraction of blood as indicated above. DNA was extracted in batches using QiaAmp blood mini kit (Qiagen GmBH, Hilden, Germany) as per the manufacturer′s instructions. The extracted DNA was stored at -20°C and used for nPCR testing. PCR testing by targeting IS6110 sequence Following extraction, a nested PCR for the detection of M. tuberculosis was performed from the DNA samples. All the PCR reagents including Hotstar Taq polymerase were procured from Qiagen (Hilden, Germany). Negative controls were included in every assay replacing the template with nuclease free water (Qiagen GmBH, Hilden, Germany). A DNA extracted from M. tuberculosis strain was used as positive control in every run. The forward and reverse external primers used for the assay were CCGGCCAGCACGCTAATTAACGGTTC and TGTGGCCGGATCAGCGATCGTGGT respectively as reported by Cheng et al. [9] by using the following cycle profile 95°C for 15 minutes, 94°C for 45 seconds, 57°C for 45 seconds, 72°C for one minute 30 seconds, 72°C for 10 minutes (after 30 th cycle). A 5μl product of the first round was used as the template for the second round. The internal forward and reverse primers were CTGCACACAGCTGACCGA and CGTTCGACGGTGCATCTG respectively with the following cycle profile 95°C for 15 min, 94°C for 45 seconds, 57°C for 45 seconds, 72°C for one minute, 72°C for 10 minutes (after 30 th cycle). All precautions were taken for PCR testing like flow through, disposable plastic ware, and gloves, filter blocked tips and dedicated micropipettes. The PCR was carried out in Eppendorf thermal cycler (Mastercycler® personal 5332, Hamburg, Germany). Analysis of amplification products An aliquot of 5μL amplicon was analysed by gel electrophoresis in 2% agarose (Sigma, MO, USA) prepared in Tris-Borate-EDTA buffer containing 0.5μg/mL of ethidium bromide (Sigma, MO, USA). The gels were examined in a gel documentation system (Genei, Bangalore, India) for a 193 bp product. Establishment of lower limit of detection for IS6110 of M. tuberculosis by plasmid cloning PCR products were produced with above cycling conditions with final extension of 10 min at 72°C. PCR products were checked by agarose gel electrophoresis for single, discrete band. TOPO TA cloning kit (Invitrogen, CA, USA) was used to clone the PCR product as per manufacturer′s instruction. Copy number of the cloned plasmids was calculated using the formula: weight of PCR fragment (in grams per mL)/ (660 g per mol × the number of base pairs of the PCR fragment) × (6.023 × 10 23 ) = the number of genome copies per microlitre. The concentration of the plasmid was determined by measuring the optical density at 260 nm with a spectrophotometer (μQuant, Biotek instruments, Inc, VT, USA). The probability of detecting M. tuberculosis in a suspension of known concentration in the presence of defined DNA copy numbers was determined essentially as described previously. [10] The cloned plasmids were serially diluted 10-fold in TE buffer (pH 8.0) within the concentration range of 10 0 to 10 9 plasmid copies/μl. The dilutions were stored at -20°C until use. The approximate number of plasmid copies/μl of DNA suspension was determined by nPCR in triplicates using appropriate negative controls. Amplification shown in the highest dilution (least concentration) was taken as lower limit of detection as plasmid copies per microlitre. Logistics of this prospective study The blood sample was directly inoculated into the blood culture bottle and the results communicated to the treating physician on a daily basis. DNA from buffy coat samples was extracted on the same day of blood collection. nPCR testing was done on archived DNA samples by batch testing. Statistical analysis The data was entered in Excel spreadsheet (Microsoft office 2007). Accuracy indices were calculated using Epi Info 6.04d version (CDC, public domain software). Results In our study subjects, males were 185 and females were 170 in number. The patients from rural community were 240 (67.6%) and from peri-urban community were 115 (32.4%). The age of the patients recruited in the study ranged from two to 81 years. Among these, two were below five, 17 between age 5 and 15 and 335 above 15 (age data not available for one volunteer). The nested PCR showed specific amplification (193 bp) of M. tuberculosis with the control strain. In experiments for determination of lower limit of detection the assay was able to detect down to 0.1 plasmid copy per microlitre. [Figure - 1] shows the gel analysis of the lower limit of detection experiment. [Figure - 2] shows the findings of the gel analysis of clinical samples tested showing a typical patient sample positive. Of 355 blood cultures, BacT/Alert 3D was positive for seven indicating mycobacterial growth and 10 grew heterologous bacteria. The nPCR detected genomic material in 24 (6.8%) individuals. None of the ten patients whose blood culture grew heterologous bacteria had nPCR positive for M. tuberculosis. [Table - 1] shows the organism obtained in blood culture. Signal indicating growth of mycobacteria was obtained in 7 (2%) of 355 samples. The blood culture broth flagged as positives by the instrument were cultured on LJ medium and held for six weeks, none of these grew the organism. The DNA extracted from the broth and examined by nPCR were negative. For the purpose of the study, a positive signal in BacT/Alert 3D MB culture bottle was taken as culture positives. The results of the comparison of blood culture findings and nPCR is shown in [Table - 2] with the accuracy indices. The sensitivity and specificity of the nPCR was 100% and 96.3% respectively. In our study, among 355 samples, 6.8% of the samples were positive in nPCR, majority of the positives were in the known HIV seropositive group. Among the 24 nPCR positive individuals, 10 (4.16%) were from rural community (n=240) and 14 (12.2%) were from peri-urban community (n=115). There was a statistically significant difference between the two (P < 0.005), the Chi 2 value being 7.91. Discussion The automated blood culture system used in our study detected seven positives for mycobacterial growth. The nPCR (IS6110) on DNA extracts from buffy coat samples was positive in 24 individuals. The seven individuals who were blood culture positive were also positive by nPCR on buffy coat samples. The nPCR thus detected 17 more individuals to be actively infected with M. tuberculosis. In India, it is opined that diagnosis of tuberculosis is primarily based on clinical features, histopathology, demonstration of acid fast bacilli (AFB) and isolation of Mycobacterium tuberculosis in culture. The available techniques have several drawbacks such as lack of rapidity and have inadequate sensitivity and specificity. More recently, several rapid techniques for early detection (5-14 days) as compared to conventional methods (two to eight weeks) have been reported. An interesting advance in culture methods was the Bactec, mycobacterial growth indicator tuber (MGIT), Septi-chek, MB/ BacT systems. The organism in culture is confirmed by rapid methods based on lipid analysis and specific gene probes, PCR-RFLP methods and ribosomal RNA sequencing. Advances in biotechnology have facilitated the development of gene probes and gene amplification methods for identification and detection of tubercle bacillus, from culture or directly in clinical specimens. The application of gene probes and gene amplification methods allows improved capability to enhance the diagnosis of tuberculosis. [11] The IS6110 as a target is suitable as it is found to be present only in members of Mycobacterium tuberculosis complex. BacT/alert 3D has been successfully employed for the recovery and identification of M. tuberculosis from clinical specimens, [12] the manufacturers recommend testing the signal positive samples by a DNA hybridization technique (Accuprobe/Gen-Probe). This confirmation technique requires separate instrumentation and reagents and adds additional cost. Overall, this automated culture system including confirmation requires 10 to 18 days. So, though the automated blood culture system is good, its use in resource-poor settings like India is limited by cost overlays. Including capital expenses, depreciation value for the equipment, consumables for sample collection, culture and identification, manpower and utilities expenses on an estimated load of 6000 samples per year, the cost works out to Rs 525/- without antibiotic sensitivity testing. Similarly, an estimated cost for nPCR is Rs 700/-. Hence, the scope of our study was to evaluate a nested PCR as a rapid alternative method for detection of M. tuberculosis. The nPCR in all, including time for sample processing, DNA extraction, two rounds of PCR and gel detection requires only 10 hours giving a definitive result in contrast to blood culture which takes many days. The sensitivity of PCR depends on many factors. Among these, the type of sample plays a significant role. The convenience of using buffy coat samples could avoid time consuming sample processing steps like for sputum. Moreover, buffy coat is the best choice of specimen as patients with pulmonary, disseminated or extra-pulmonary tuberculosis would have mycobactereamia. M. tuberculosis is reported to infect monocytes and can hence be detected from peripheral blood. The buffy coat fraction is enriched with monocytes derived from blood. In our study, the nPCR was more sensitive than previously reported. It has been reported that the diagnostic sensitivity of TB PCR was 75.9% in culture confirmed cases and 81.3% in clinically diagnosed patients. [9] Subsequently, a study from India showed 63% of 191 samples to be positive by PCR. In 140 of these samples, wherein the conventional techniques were found negative, 74 (53%) samples were positive by PCR alone. Among 51 samples positive by conventional techniques, 46 (90%) were found positive by PCR. [13] We have not only used buffy coat sample extracts, but also used Hotstar Taq in the two rounds of nPCR. Thus, combining the use of an improved nested PCR and buffy coat samples substantially increased the rate of detection in the population. This is in accordance with Flores et al. [14] who identified that the use of IS6110 as a target and the use of nested PCR to have significantly higher diagnostic accuracy compared to other targets and methods. However, the study was done on sputum samples. IS6110 PCR was also evaluated in clinical samples such as sputum, blood and faeces. In whole blood, the detection limit was 20 cells per microlitre. [15] The authors, however, used a non-nested format. In our study, the detection limit was less than 1 plasmid copy per microlitre using Hotstar Taq and nPCR format. M. tuberculosis is a true pathogenic bacterium with greater capacity for causing disseminated disease. [5] Mycobacteraemia is commonly observed in HIV positive patients. [16] The lysis of peripheral blood leukocytes releases intracellular mycobacteria, which are concentrated by centrifugation, increasing the sensitivity of blood culture [17] indicating the value of buffy coat cells as a source of M. tuberculosis in cases of mycobacteraemia. This has been proved by several studies involving isolation of M. tuberculosis from peripheral blood leukocytes. [18] In order to process blood for Mycobacterium culture, simple and inexpensive techniques such as lysis-centrifugation method have been described. [5] In this method, sodium deoxycholate solution was used for lysis followed by centrifugation at 3000g for 30 min and inoculation in the medium. However, the yield of isolation was similar to that of direct inoculation. Using lysis-centrifugation technique, mycobacteraemia was detected in HIV and non-HIV patients by David et al. [19] followed by subculture in LJ medium. They suggested this technique as a useful adjunct to diagnose TB. In the BacT/Alert 3D system, lysis of blood cells is facilitated to achieve a similar effect. MB/BacT enrichment fluid contains components which were necessary to ensure optimal growth of mycobacteria and contains a lytic agent for blood cell lysis. A comprehensive study has been published recently showing the advantage of automated culture system. The authors report their experience with Bactec 460 TB system over a five-year period comparing its performance characteristics with the conventional LJ medium for mycobacterial culture. A total of 3597 clinical specimens from patients suspected to have tuberculosis were processed for mycobacterial culture using the Bactec 460 TB system. A total of 1568 pulmonary samples and 2029 extra pulmonary samples were processed. A detection rate of 18.93% with a recovery time shorter by 13.2 days by Bactec was achieved, which was significantly superior to the conventional method. [20] Our study was on the use of a molecular detection, exploring yet another facet to improve the diagnostics for tuberculosis. In our opinion, the nested PCR, using Hotstar Taq for the detection of IS6110 sequence of M. tuberculosis in buffy coat DNA extracts, used in our study was found to be a very useful technique and its further evaluation in large multicentre studies would validate this technique for application in clinical settings. Acknowledgment This work forms a part of the Ph.D. thesis work of Sri N. Balaji. The funding by the Division of Biomedical Research of SNHRC is gratefully acknowledged. Authors are indebted to Dr. Rajesh Kannangai (Christian Medical College, Faculty of Clinical Virology, Vellore, India) for facilitating cloning related experiments. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10069f2.jpg] [mb10069t2.jpg] [mb10069t1.jpg] [mb10069f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}