 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
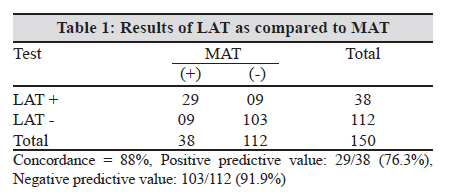
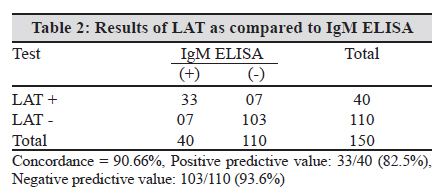
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 238-240 Brief Communication Comparison of an in-house latex agglutination test with IgM ELISA and MAT in the diagnosis of leptospirosis S Shekatkar, NS Acharya, BN Harish, SC Parija Department of Microbiology, JIPMER, Pondicherry, India Keywords: Leptospirosis, latex agglutination test, microscopic agglutination test, IgM ELISA, diagnosis Introduction The clinical diagnosis of leptospirosis is inaccurate and frequently gets confused with other similar febrile illnesses. The early diagnosis of the disease reduces the mortality and morbidity. Enormous progress has been made in laboratory diagnosis of leptospirosis in the last few decades. But the need for a quick, simple, reliable and affordable diagnostic test for leptospirosis is still elusive. [1] In leptospirosis, antibodies usually appear within five to seven days after onset of symptoms and persist in detectable levels for many months. [2] From the patient and also physician point of view early detection of disease is desirable. The most commonly used tests are IgM ELISA as well as MAT. These tests are sensitive and specific, but are expensive and laborious to perform. Hence, there is need to develop a simple, rapid test for screening for anti-leptospiral antibodies. The main objective of the present study was to standardize and compare the efficiency of an in- house latex agglutination test (LAT) with a commercially available IgM ELISA and microscopic agglutination test (MAT). Materials and Methods Blood samples were obtained from 150 patients suspected of leptospirosis attending our hospital from January 2007 to April 2008. Serum was separated and stored at -20°C until use. Leptospiral antigens Five locally prevalent leptospiral strains, Leptospira interrogans serovars Australis (strain Ballico), Canicola (strain Hond Utrecht IV), Icterohaemorrhagiae (strain RGA), Pomona (strain Pomona) and Leptospira kirschneri serovar Grippotyphosa (strain Moskva V) were grown in liquid EMJH medium for 7-10 days. The medium was then centrifuged at 10,000 rpm for 20 minutes, pellets collected, washed and re-suspended in 0.06M carbonate buffer. The cells were then sonicated using sonicator (Vibracell) at 20Hz for two periods each of 15 seconds. Hyper immune serum was raised against each of the above mentioned five serovars in duplicate healthy rabbits using standard protocol. [3] Sensitisation of latex beads Latex beads (0.8μ diameter, Sigma USA) were washed in 0.06M carbonate - bicarbonate buffer, pH 9.6 twice by centrifugation at 8000rpm for 2minutes each time. 10% of this was coated with equal volume of pooled leptospiral antigen using 0.06M carbonate - bicarbonate buffer and kept at 37 o C for six hours with constant shaking. The sensitized beads were centrifuged at 8000 rpm for three minutes and the pellet was re-suspended as 1% suspension in PBS pH 7.2 containing 5mg/ml of bovine serum albumin (BSA). The latex beads were left overnight at 37 o C with constant shaking. They were centrifuged as before and re-suspended in PBS pH 7.2 containing 0.5mg/ml of BSA and 0.1% sodium azide as 0.25% suspension. This was kept at 4 o C until use. [4] Latex agglutination test LAT was performed on black agglutination cards by mixing equal volume of serum and sensitized beads (20μL each). The card was rocked for 5-10 minutes. The test was considered positive if agglutination occurred indicated by fine granular particles and test was said to be negative if the suspension remained homogenous. Positive and negative controls were included with each batch of test done. Hyper immune rabbit antiserum against the above mentioned strains using standard protocol was used as positive control and serum from a healthy rabbit served as negative control. IgM ELISA It was performed using the IVD LEPTOSPIRA IgM Microwell ELISA Test (IVD Research Inc, Carlsbad, CA92010 USA, as per the manufacturer′s instructions. The absorbance of positive and negative control serum provided in the kit was used for calculations. A negative result was defined as an absorbance of 0.0-0.3 optical density (OD) units, an equivocal result as 0.5 to ≤1 OD units and a positive result as >1.0 OD units. Microscopic agglutination test The gold standard serodiagnostic test for leptospirosis is MAT, which was performed as per the method of Cole et al. [5] Briefly, the sera to be tested were diluted serially from 1 in 50 to 1in 3200 in phosphate buffered saline (PBS) pH 7.2. Live leptospiral antigen suspensions from a battery of 12 serovars were added and allowed to incubate at 37 o C for two hours. The serum antigen mixtures were then examined by darkfield microscopy for the presence of agglutination or clearance and the titres were determined. Reciprocal agglutination titres of ≥ 100 were taken as positive. The relative sensitivity and specificity of the LAT for the detection of leptospiral antibodies was determined in comparison with MAT and IgM ELISA. Results The latex test was done with the sonicated antigen from five locally prevalent leptospiral serovars. Out of 150 samples tested, 38 turned out to be positive by LAT. In comparison with MAT, the relative sensitivity and specificity of LAT was (90.62%) and (91.96%) [Table - 1]. In comparison with IgM ELISA, out of the 150 samples tested, 40 were positive and 110 were negative by LAT. The relative sensitivity was (82.5%) and specificity was (93.63%) [Table - 2]. Discussion Leptospirosis is a disease of tropical countries, where it often is endemic, but may also occur in epidemics. Laboratory diagnosis is necessary to confirm the diagnosis of clinically suspected leptospirosis due to its varied symptoms. The laboratory tests are mainly based on serological methods, and the most widely used reference standard method, MAT, has many disadvantages. Rapid and easy to perform tests are valuable in endemic situations and during outbreaks, where a large number of patients have to be tested. IgM ELISA is one such test, which is popularly done for the diagnosis of acute leptospirosis. The cost of the test and requirement of specialized equipments still restricts the use of IgM ELISA in well equipped laboratories only. The LAT potentially can be used outside the laboratory and can be done for individual samples without the need of batch testing and so it may help to improve the healthcare of people in endemic areas. The centre of attention of the present study was to develop a rapid diagnostic test for the diagnosis of leptospirosis by using locally prevalent leptospiral serovars as antigen. The result of the LAT test showed good sensitivity and specificity i.e. sensitivity (90.62%) and specificity (91.96%) when compared with MAT and 82.5% and 93.63% sensitivity and specificity respectively as compared with IgM ELISA, which was also observed in other studies. Senthilkumar et al. used a recombinant rLipL41 antigen for latex agglutination and the overall sensitivity and specificity of this test when compared to MAT was found to be 89.7% and 90.45% respectively. [4] Smits et al. using a heat-stable, broadly reactive antigen prepared from the pathogenic strain Lely 607 standardized a latex agglutination test and 82.3% sensitivity and 94.6% specificity was seen. [6] It is significant to note that in this study though crude antigens have been used, the test has given reasonably good sensitivity and specificity. This implies that this test could be a good alternative in laboratories where facilities and resources for refining and recombination of antigens is not possible. The results of this study further show that the latex agglutination assay could be a valuable tool in the diagnostic armament for leptospirosis. The assay is simple and rapid to perform, uses stabilized components, and can be performed without the need for training or special or expensive equipment. The assay is sensitive and results are concordant with those of the IgM ELISA and MAT. Together, these test characteristics make the assay suitable for use in situations were facilities or resources to perform more complicated tests are not available. The assay also gives a quick result, which can be important in the management of patients, especially when attention must be given to a large number of patients. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10071t2.jpg] [mb10071t1.jpg] |
| |||||||||

{kind=link}
{kind=link}