 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
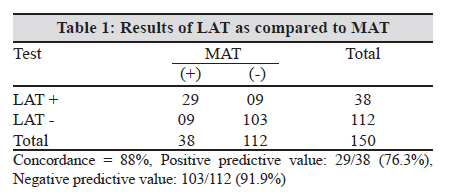
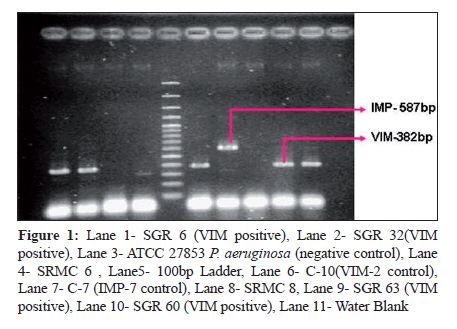
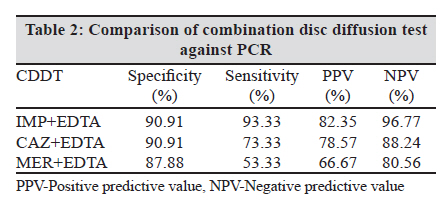
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 241-244 Brief Communication Detection and characterization of metallo beta lactamases producing Pseudomonas aeruginosa A Manoharan1, S Chatterjee1, D Mathai1, SARI Study Group2 1 Benjamin M Pulimood Laboratories for Infection, Immunity and Inflammation (BMPLIII), Department of Medicine Unit I and Infectious Diseases, Christian Medical College, Vellore -632004, Tamil Nadu, India Keywords: Carbapenem, E test, PCR, Pseudomonas, Resistance Introduction Pseudomonas aeruginosa isolates are responsible for outbreaks of nosocomial infections in different parts of the world. These isolates have also been responsible for serious infections such as septicemia and pneumonia. P. aeruginosa resistant to carbapenem, [1] currently the most effective treatment option is being increasingly reported. [2] Resistance to carbapenems is often mediated by production of Metallo-Beta-Lactamase (MBL), a class B type of beta-lactamases that require bivalent metal ions, usually zinc for their activity. [3] P. aeruginosa, producing MBLs, was first reported from Japan in 1991 and since then has been described from various parts of the world, including Asia, Europe, Australia, South America, and North America. [4],[5] In some countries, P. aeruginosa possessing MBLs constitute nearly 20% of all nosocomial isolates. [6] In India, published reports indicate the prevalence of MBLs to range from 7-65 % [7] with a recent study reporting 34% occurrence. [8] Several phenotypic methods are available for the detection of MBL-producing bacteria. All these methods are based on the ability of metal chelators, such as EDTA and thiol-based compounds, to inhibit the activity of MBLs. These tests include the double-disk synergy tests using EDTA with imipenem (IMP) or ceftazidime (CAZ), 2-mercaptopropionic acid with CAZ or IMP , Hodge test, a combined disk test using EDTA with CAZ or IMP, the MBL Etest (bioMerieux Marcy l′Etoile, France) , and a microdilution method using EDTA and 1,10-phenanthroline with IMP. [1] The double-disk synergy test and Hodge test are often difficult and subjective to interpret. These tests can also be technically demanding and time-consuming, since optimal disk spacing and reincubation of plates are sometimes required to obtain ideal results. Further, 2-mercaptopropionic acid and 1, 10-phenanthroline are toxic for routine handling, and special precautions have to be taken when working with these compounds. [1] These methods are thus unsuitable for clinical laboratories to perform on a routine basis. So far no studies from India have compared phenotypic and molecular method for screening and confirmation of MBLs. The objective of the present study was to evaluate Combined Disc Diffusion Test (CDDT) with confirmatory Etest and PCR. Material and Methods Bacterial strains The study reference laboratory (BMPLIII) received >700 isolates from different centres participating in the seven centre Surveillance of Antimicrobial Resistance Study (SARI) during 2005-2007. From 176 P. aeruginosa strains received, 61 (>80% from respiratory, skin and soft tissue and urine) were selected based on clinical significance and evaluated for CARB-R and MBL production. The strains were confirmed biochemically using standard methods. Antimicrobial susceptibility testing Resistance to IMP, MER and CAZ was determined by Kirby Bauer disc diffusion testing with using CAZ (30μg), IMP (10μg), and MER (10μg). The zones of inhibition were interpreted as per CLSI (M100-S15) 2007. The quality control strains used for the study were Escheichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853. Screening for and confirmation of MBLs The strains resistant to ceftazidime and carbapenems were screened for MBL by CDDT using CAZ (30mg) + 5ml-0.5M EDTA (930mg), IMP (10mg) + 5ml-0.5 M EDTA(930mg) and MER (10 mg) + 5ml-0.5 M EDTA(930mg). An increase of 7mm or more in zone diameter in the presence of EDTA compared to those with IMP, MER or CAZ tested alone was considered to be a positive test for the presence of an MBL. [1] MBL production was further confirmed by IMP + IMP-EDTA Etest strips (bioMerieux Marcy l′Etoile, France). Manufacturer′s directions were followed for interpretation of results. Additionally colistin Etest was done on MBL- producing P. aeruginosa. MBL gene identification DNA template preparation was performed as follows; Fresh Culture of the test organism and the control strains were suspended in 500ml of saline and vortexed to get a uniform suspension. The cells were lysed by heating them at 100°C for ten minutes, and cellular debris was removed by centrifugation at 8000 rpm for five minutes. The supernatant was used as a source of template for amplification. Duplex PCR amplification for the simultaneous detection of IMP and VIM MBL genes were carried out on a Thermal Cycler 9700 instrument (Applied Biosystems, Norwalk, Conn.).The master mix for the PCR was prepared as follows: 2.5ml of PCR buffer, 2.5ml of 25mM MgCl 2 , 2.5ml of 2mM DNTPs, (Fermantas, Glen Brunie, MD) 8.2ml of MilliQ H 2 O, 1ml of each of the forward and the reverse primers and 0.3ml of Taq Polymerase (Fermantas, Glen Brunie, MD). Finally, after dispensing 20ml of the master mix in the individual amplification tubes, 5ml of the extracted DNA was added in the corresponding tubes, the total volume being 25ml. The PCR programme included an initial denaturation step at 94°C for two minutes followed by 30 cycles of DNA denaturation at 94°C for one minute, primer annealing at 54°C for one minute and primer extension at 72°C for one and half minutes with a holding temperature of 72°C for five minutes. After the last cycle the PCR products were stored at 4°C. The PCR products were analyzed by electrophoresis with 1.5% Agarose gels in TBE buffer. The gels were stained with ethidium bromide and the PCR products were visualized under UV light. The primers used for the amplification of the VIM type of MBLs at a concentration of 20 picomolar each were VIM2004A (5′-GTT TGG TCG CAT ATC GCA AC-3′) and VIM2004B (5′-AAT GCG CAG CAC CAG GAT AG-3′) which amplified a 382-bp amplicon. The primers used for the amplification of the VIM type of MBLs at a concentration of 20 picomolar each were IMP-A (5′-GAA GGY GTT TAT GTT CAT AC-3′) and IMP-B (5′-GTA MGT TTC AAG AGT GAT GC-3′) which amplified a 587bp amplicon. (Y = C or T and M = A or C). [1] The presence of VIM and IMP was detected in the clinical isolates of CARB-R P. aeruginosa. C-10(VIM-2) and C-7(IMP-7) were used as positive controls for the study. Results Antimicrobial susceptibility of P. aeruginosa Among the 61 P. aeruginosa isolates, resistance to CAZ or IMP or MER was 42.6%. These isolates were further tested for MBL production. Screening for MBLs using EDTA disk screen Tests and MBL Etest Of the 61 P. aeruginosa clinical isolates included in this study, 20 were confirmed to be MBL producers by the IMP + IMP-EDTA Etest. Among the CDDT combinations, results were more clearly discernable for the IMP + IMP- EDTA combination using the ≥7mm cut off. The mean zone diameter for IMP for MBL producers was 7.35mm and with EDTA was 20.05mm. The non MBLs had a mean zone diameter of 21.66mm for IMP and in combination with EDTA was 22.49mm. [Table - 1] gives the comparison of the three different CDDT combinations against the confirmatory Etest. None of the screening methods showed complete correlation when compared to confirmatory Etest. The IMP + EDTA had the highest specificity and sensitivity for detection of MBLs as compared to the others. Colistin Etest The 20 MBL producers were susceptible to colistin with MIC ranging from 0.5- 0.032ug/ml. PCR for IMP and VIM PCR testing detected VIM type of MBL among 15 of the 48 tested isolates; all were negative for IMP MBL gene [Figure - 1]. Of the 20 MBLs confirmed by Etest, 17 were available for PCR testing, 15 were VIM positive and two isolates were negative for both IMP and VIM. [Table - 2] gives the comparison of CDDT to PCR testing; the IMP + EDTA had higher specificity and sensitivity for detecting MBLs as compared to others. Discussion MBL production is a significant problem in hospital isolates of P. aeruginosa. With increasing isolation of ESBL-producing isolates in the hospital setting necessitating the use of carbapenems, the problem of MBL production is also increasing. The development of simple screening tests designed to detect acquired MBL production is a crucial step towards large scale monitoring of these emerging resistant determinants. Though there are several screening methods recommended for the detection of MBL production, no single test when used alone is specific for these enzymes. A recent study [7] has supported the present study findings and recommended use of imipenem and imipenem + EDTA disc diffusion screen. The disc diffusion screen has been further validated against a PCR and has been found to outperform ceftazidime and meropenem EDTA combination. It may not be practically possible for all laboratories to perform the Etest due to cost constraints and availability; however the CDDT should not be very difficult to implement. In our study, all imipenem-resistant isolates had detectable MBLs, however, there are other resistance mechanisms involved, such as permeability mutations via the loss of porins or the up-regulation of efflux systems, which may be missed by the Etest or the MBL PCR. We had previously reported novel VIM type of MBL-producing Pseudomonas spp. detected in India during 2006 in which strains were clustered in 33 ribotypes with clones found in multiple hospitals. Several types of VIM-2-carrying integrons were detected including a newly characterized variant, VIM-18 which showed a 4-amino-acid deletion compared to other VIM variants. [8] The present study also shows that only VIM type of MBL to be present among the study strains. It is impossible to predict what impact MBL genes will have on the future antimicrobial regimens. There is little doubt that in India the number of MBL possessing P. aeruginosa infections are such that the mainstay antibiotic regimens used to eradicate these bacteria can no longer be relied upon. Our results support the important role that clinical microbiology laboratories must play to be able to distinguish MBL-producing P. aeruginosa from strains with other mechanisms responsible for carbapenem resistance. The early detection of MBL-producing P. aeruginosa may help in appropriate antimicrobial therapy and avoid the development and dissemination of these multi drug resistant strains. We recommend that all ceftazidime and imipenem/meropenem-resistant P. aeruginosa isolates be routinely screened for MBL production using IMP + IMP-EDTA disk screen test. Acknowledgements Authors are grateful to CIPLA India for funding the SARI study and CMC IRB for approving conduct of this study vide min no.5925 dt 20th June 06. Authors thank Dr.JD.Pitout, University of Calgary, Canada for sharing the quality control strains C-10 (VIM-2) and C-7 (IMP-7) used in this study. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10072t2.jpg] [mb10072t1.jpg] [mb10072f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}