 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
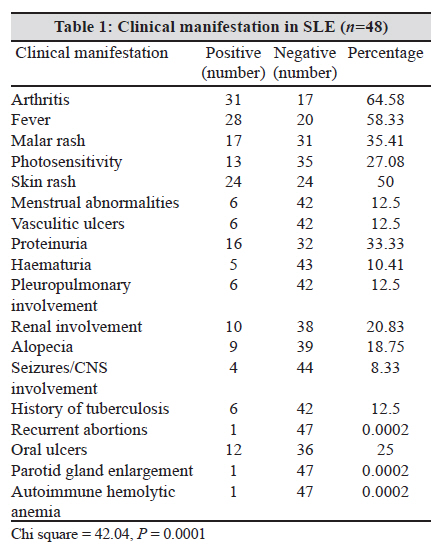
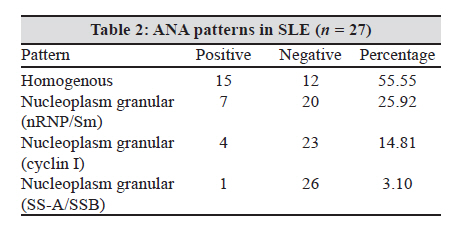
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 245-247 Brief Communication A cross-sectional hospital-based study of autoantibody profile and clinical manifestations of systemic lupus erythematosus in south Indian patients K Kosaraju, S Shenoy, U Suchithra Kasturba Medical College, Light House Hill Road, Mangalore, Manipal University - 575 001, India Keywords: ANA profile, anti dsDNA, antinuclear antibodies, systemic lupus erythematosus Introduction Systemic lupus erythematosus (SLE) is a prototypic autoimmune disease characterized by the production of antibodies to components of the cell nucleus in association with a diverse array of clinical manifestations. [1] The basic pathological features of SLE include band or occlusive vasculopathy, vasculitis, and immune complex deposition. The best characterized organ pathology is in kidney. Nephrotic syndrome occurs in 13-26% of patients with active lupus nephritis. [2] The central immunological disturbance in patients with SLE is autoantibody production. Autoantibodies found in SLE patients are antinuclear antibody (ANA), antidsDNA antibody and anti-extractable nuclear antigen (ENA) antibody. Anti-ENA antibodies include anti-Smith (Sm), anti-ribonucleoprotein (RNP), anti-Ro and anti-La antibodies. [3] Since SLE is a rare disease, a general physician is not likely to be familiar with the complexities of its presentation and the therapeutic challenges and dilemmas it can pose. Therefore, Aim of our study was to determine the frequency of various auto-antibodies that are found in our geographic area and to ascertain the clinical manifestations that can be found in our SLE patients. Materials and Methods A cross sectional study was conducted for a period of 16 months (September 2006 to January 2008) after gaining approval from institutional ethical committee. Study population included both young and adult patients, both inpatients and out-patients, presenting to General Medicine, Dermatology and Orthopaedic departments of our hospital. Patient details - age, gender, religion, occupation, residential address, chief complaints, significant past history, treatment and family history were noted. Vital signs were recorded and any significant findings on systemic examination were noted. Forty eight SLE patients who were diagnosed based on the revised criteria for the classification of systemic lupus erythematosus were included in the study. About five ml of the venous blood was collected from the antecubital vein, under strict aseptic precautions, into a vaccutainer. Serum was separated and processed immediately or stored at - 80°C in case of delay. Non-specific Laboratory tests like Haemoglobin estimation, Total and differential leukocyte counts, ESR estimation and Peripheral blood smear examination were performed by an automated method (automated Haematology analyser Sysmex XT-1800i, Sysmex corporation, Kobe, Japan). Detection of ANA was done by indirect immunofluorescence using a commercial kit (EUROIMMUN Medizinische Labordiagnostika AG, D-23560 Lubeck (Deutschland) Seekamp). Dilution of serum used was 1:100 as per manufacturer instructions. An Indian study reports that optimal dilution of 1:80 would be economical and valid to distinguish from healthy individuals. [4] Also since titres do not correlate with disease activity, serial measurements were not indicated. [5] Antibodies to dsDNA were detected by indirect immunofluorescence using Crithidia luciliae flagellates as substrate using a Commercial Kit (EUROIMMUN Medizinische Labordiagnostika AG D-23560 Lubeck (Deutschland) Seekamp). Antibodies to different antinuclear antigens were detected by using immunoblot strips (EUROIMMUN Medizinische Labordiagnostika AG, D-23560 Lubeck (Deutschland) Seekamp) coated with 14 different antigens: nRNP, Sm, SS-A (SS-A native and Ro-52), SS-B, Scl-70, PM-Scl, Jo-1, CENP B, PCNA, dsDNA, Nucleosomes, Histones, ribosomal P-Protein and AMA-M2. Frequency of autoantibody detection and clinical manifestations were reported in percentage over total sample size (forty-eight subjects) and was analyzed statistically by chi-square and P value. Results Clinical manifestations were studied in 48 patients as shown in [Table - 1]. Arthritis was the most common clinical manifestation (64.58%); followed by fever (58.33%) and skin rash (50%). Renal involvement in the form of lupus nephritis was seen only in 20.83% of patients. Mean age at onset of disease was 34.25 years (range 12-70 years). Female to male ratio was 15:1, with peak ratio in the age group of 21-30 years. ANA was positive only in 27 patients and anti-dsDNA was positive in 89.36% of patients with clinical diagnosis of SLE. Homogenous pattern was most common [Table - 2]. ANA profile showed positive reactions with dsDNA, RNP and Sm antigens. Discussion Arthritis was the most common clinical manifestation in SLE [Table - 1] similar to a south Indian study. [6] Malar rash was seen less frequently than reported in the above study. Dark complexion of skin in Indians makes it difficult to detect the rash, which explains the rare observation in Indian studies. Vasculitic ulcers were seen less commonly in our patients [Table - 1], and in accordance to an Indian study, [7] cutaneous vasculitis was associated with neuro-psychiatric lupus, seizures and organic brain syndrome. Clinical features reported by workers from different parts of India show some interesting regional variations. Arthritis is most commonly seen in south and eastern India than the other parts. It is evident that oral ulcers are seen in about one-half of patients at presentation in those from eastern India as against about 10% from other parts (25% in our study). Raynaud′s phenomenon is conspicuous by its absence in patients from southern India. Nephritis in SLE is more common among South East Asian than in Indian patients. However, it is seen more in eastern india and is rare in south and north Indian population. [8] These regional variations in the occurrence of clinical manifestations, probably HLA-linked, explain the findings of the present study from south India. Fifteen patients (31.25%) were in the age group of 21-30 years (Median age = 30 years). All patients were above 13 years of age and only six patients were in the age group of 13-20 years. Female to male ratio was 15:1, with peak ratio in the age group of 21-30 years. In two Indian studies, [9],[10] median age of onset was at 24 and 26 years respectively. This increased frequency of SLE among females is thought to be due to hormonal effects. We did not observe any increasing complications in men with SLE as when compared with female counterparts. ANA was positive in 64.28% and anti-dsDNA was positive in 89.36% of patients, in contrast to a study, [6] which reported positive ANA by Immunofluorescence in 93.3% and positive dsDNA by ELISA in 76%. Low positivity of ANA in our study could be due to a small subgroup of patients with ANA negative lupus or levels of ANA could be too low in the sera to detect by these assays and also our follow up period may not have been long enough to detect further development of ANA in these patients. [11] Anti-dsDNA is the hallmark of SLE, likewise, in the present study also, the occurence of 89.36% positivity in clinically diagnosed SLE coincides with this fact. Homogenous pattern was the most common among patients with SLE [Table - 2]. Sera from eight patients with clinical diagnosis of SLE and positive ANA by immunofluorescence were further evaluated for ANA specificities by immunoblotting. Four samples (50%) were positive for RNP, Sm antigens and six (75%) for dsDNA. All patients with lupus nephritis were positive for dsDNA (100%) coinciding with the fact that antibodies to dsDNA are strongly associated with renal involvement in patients with lupus. [12] Antibodies to RNP, Sm were found only in 50% of lupus nephritis which was similar to a histological and immunopathological study [13] which reported a positive RNP antibody by counter-immunoelectrophoresis in patients with severe renal disease. dsDNA was most common reactivity identified at all intensities of immunofluorescence (3+, 2+, 1+). Raised ESR was seen in 97.77% of patients whereas a raised CRP was seen only in 55.55% of patients. It is proposed that inflammation in SLE, in contrast to inflammation in other rheumatic diseases, is characterized by elevated ESR while CRP often remains low. [14] On follow-up, prognosis was good in our study and could be attributed to high suspicion, early diagnosis and effective treatment regimens. According to findings from the present study, we observed that clinical manifestations can vary ranging from a typical malar rash to atypical involvement of CNS and geographic location of the patients determines the most likely clinical presentation and therefore, can guide the physicians in identifying disease at an early stage. Though detection of ANA is an important screening test, identification of antibodies against dsDNA, RNP/Sm has more reliable diagnostic and prognostic implications because high levels of dsDNA, RNP/Sm are seen in patients with active renal lupus and contribute to pathogenesis of lupus nephritis. [15] Owing to its chronicity and ability to cause serious complications, early detection, diagnoses and management might go a long way in delaying serious systemic involvement. However, studies on clinical features and autoantibody profiles involving a larger population are required to validate the findings of the present study. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10073t1.jpg] [mb10073t2.jpg] |
| |||||||||
{kind=link}
{kind=link}