 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
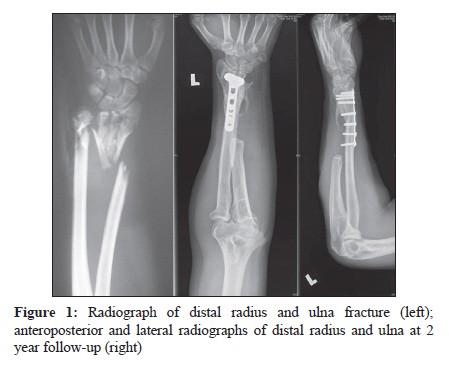
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 248-250 Case Report Mycobacterium chelonae and Mycobacterium fortuitum infection following open fracture: A case report and review of the literature K Kwan1, ST Ho2 1 Department of Orthopaedics and Traumatology, Queen Mary Hospital, Hong Kong Keywords: Atypical mycobacteria, infection, open fracture, trauma Introduction Osteomyelitis after an open fracture is common in young adults and but nontuberculous osteomyelitis is very rare. We report a case of open fracture after polytrauma, which was complicated by dual infection - with Mycobacterium chelonae and Mycobacterium fortuitum - in an immunocompetent patient. Case Report A 35-year-old man was injured after falling six floors. He sustained multiple fractures, including open fractures of the left distal radius and ulna [Figure - 1], right scaphoid, right femoral shaft, maxilla, and mandible, as well as closed fractures of the right patella and multiple ribs. He had no visceral or brain injuries. Immediately following resuscitation, debridement of open fractures, intramedullary nailing of the femoral shaft, tension band wiring of patella, and percutaneous K wire fixation and application of an external fixator to the left distal radius and ulna were performed. One week after the injury, the patient underwent fixation of the maxilla and mandible, percutaneous screw fixation of scaphoid, and open reduction and internal fixation (ORIF) of the distal radius with locking compression plate and re-application of the external fixator. The external fixator was removed on day 29. There persistent discharge from the left distal forearm wound. Wound swab did not reveal any microorganism even after prolonged incubation. In view of the clinical evidence of infection, wound debridement was carried out, with excision of the distal ulna and removal of the K wire on day 37. He was empirically commenced on intravenous cefuroxime. The histology report revealed granulation tissue with patchy aggregates of degenerated polymorphs. Ziehl-Neelsen stain was positive. Bacterial culture of the granulation tissue from the ulna identified Mycobacterium chelonae and a repeat wound swab grew Mycobacterium fortuitum. No other organisms were identified. Empirical antituberculous chemotherapy with rifampicin, pyrazinamide, and isoniazid were commenced on day 54. M chelonae was tested sensitive to amikacin, cefoxitin, clarithromycin, doxycycline, and levofloxacin; M fortuitum was tested sensitive to amikacin, clarithromycin, imipenem, levofloxacin, and tetracycline. Sensitivity test was performed by the standard broth dilution method. Final identification and sensitivity testing were performed by the Mycobacteriology Reference Laboratory (Public Health Laboratory Centre). The antibiotics were changed to levofloxacin and amikacin when the sensitivity results became available on day 60. Despite appropriate antibiotics there was persistent infection, and radiological evidence of impending implant failure. Debridement and revision plating were performed on day 77. The patient underwent three further debridements subsequently but the infection did not subside. He developed a left axillary mass and subcutaneous nodules in the forearm. Fine needle aspiration of the axillary mass showed mycobacterial infection on histological examination. The patient eventually underwent a radical debridement, including resection of the distal third of ulna, and drainage of his axillary abscess on day 148. He was treated with intravenous amikacin for 4 months, and oral clarithromycin for 2 months after his discharge. All wounds healed, and he was discharged after 7 months of hospitalization. At 2-year follow-up, all the fractures had healed [Figure - 1]. His forearm had full supination, pronation at 30° , and dorsiflexion and palmar flexion at 80° . He returned to light duty at work. Discussion Although osteomyelitis is a known complication of open fracture, nontuberculous infections are very rare. To the best of our knowledge, this is the first description of a case of osteomyelitis due to dual, nontuberculous mycobacterial infection following trauma. In 1959 Runyon described four groups of nontuberculous mycobacteria (NTM) according to pigment production and rate of growth. [1] Both M chelonae and M fortuitum belong to group IV, the rapid growers, which are defined as those showing visible growth within 7 days on subculture on Lφwenstein-Jensen medium. NTM are found in the environment in soil and drinking water. Animal reservoirs appear to be of lesser importance, although M chelonae has been found in fish and frogs, and M fortuitum in birds. Even though contact with environmental mycobacteria is regular and frequent, overt disease is uncommon due to their low virulence. The risk of osteomyelitis increases after open fracture in a trauma setting. The organism may reach the bone through the bloodstream, through extension of contiguous infection, or by direct traumatic introduction. Traumatic inoculation of bacteria into the bone or surrounding tissue precedes osteomyelitis. The contaminated inoculum is usually polymicrobial. The combination of tissue injury, vascular damage, oedema, haematoma, dead bone fragments, and an open pathway to atmosphere increase the chance of invasion. A larger series of NTM osteomyelitis have been previously reported in the sternum after cardiac operations [2] and in the vertebrae. [3] There are also case reports of NTM osteomyelitis involving other bones, such as the tibia after intramedullary nailing, [4] the distal femur after arthroscopy, [5] the cuboid after nail puncture wound, [6] and the proximal humerus after open fracture. [7] Immunocompromised patients, such as those on long-term steroids or those infected with HIV, are also at increased risk of developing NTM osteomyelitis. The diagnosis of NTM osteomyelitis can often be delayed in previously healthy and immunocompetent patients. Delays in diagnosis ranging from 8 months [8] to 7 years [5] have been reported in the literature. Surgeons need to consider this possibility when the clinical and histological findings are suggestive of infection but routine cultures are negative. The detection of NTM by microscopy has sensitivity between 22% and 78%. However, even routine culture characteristics may not provide a definitive identification. In a Swiss External Quality Control study, only 26% of the 50 participating laboratories identified ′rapidly growing mycobacteria′ or ′M fortuitum′ in the proficiency testing sample. [9] Amplification of mycobacterial DNA with the use of polymerase chain reaction has proven to be more sensitive than conventional detection methods. Cases of dual mycobacterial infections are rare and even more difficult to diagnose. It also has ramifications in terms of the antimicrobial regimen since each microorganism has different antibiotic sensitivities and it is not possible to determine the contribution of each species to the disease process. Ganesan described a case of dual infection, with tuberculous and NTM cervical lymphadenitis in a child who was treated with both excisional biopsy and antituberculous agents. [10] In cases of NTM osteomyelitis, patients normally require repeated debridement along with appropriate antimicrobial treatment. In some cases more radical surgical procedures, involving muscle flaps, have been used. Only one case has been reported in the literature in which the infection responded to chemotherapy alone. [8] The optimal antimicrobial therapy for M chelonae and M fortuitum consists of a combination of aminoglycosides, clarithromycin, and linezolid. The optimal duration of therapy is unknown but probably should be for at least 6 months. To conclude, this case calls attention to a rare group of organisms which can cause osteomyelitis in an open fracture. It demonstrates that a high degree of suspicion, an adequate knowledge of diagnostic procedures, and a radical treatment regimen (with surgical excision of the infected bone, debridement, and appropriate antibiotics) are required to eradicate such infections. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10074f1.jpg] |
| |||||||||
{kind=link}