 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
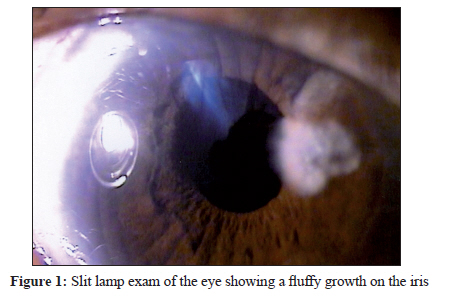
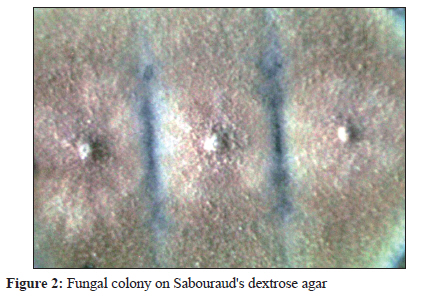
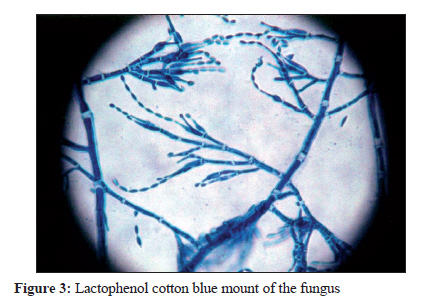
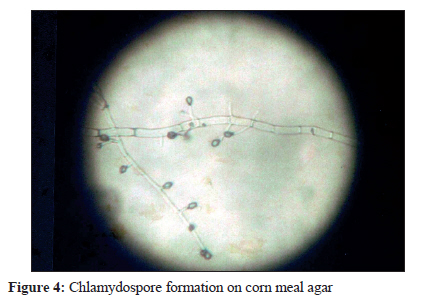
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 253-254 Case Report Fungal endophthalmitis caused by Paecilomyces variotii, in an immunocompetent patient, following intraocular lens implantation KB Anita1, N Fernandez1, R Rao2 1 Department of Microbiology, A.J. Institute of Medical Sciences, Kuntikana, Mangalore-575004, India Keywords: Endophthalmitis, ocular infections, Paecilomyces variotii Case Report The patient was a 70-year-old immunocompetent man who underwent extra-capsular cataract extraction with an intraocular lens implantation, in the right eye. He was admitted to our institution with diminished vision, signs of acute iritis, and a fluffy mass on the iris 4 months later, and was treated with topical corticosteroids. The mass was removed and sent for fungal studies. Direct microscopy of the fluffy mass revealed structures resembling fungal hyphae. The specimen was put up for fungal culture on modified Sabouraud′s dextrose agar with antibiotics. By the third day there was growth of floccose white colonies that gradually turned tan colour on the obverse and a light brown on the reverse. A lactophenol cotton blue mount of the isolate showed fungi resembling Penicillium but with phialides that were flask shaped and had elongated tapered necks, bearing chains of elliptical conidia. Microscopic studies on the slide cultures of the isolated fungus showed a similar picture. Within 2 weeks, the growth on the iris recurred; a sample from the anterior chamber was collected and sent for fungal studies. In the operating theatre, the specimen was inoculated on to modified Sabouraud′s dextrose agar with antibiotics, and brain hearth infusion broth. The modified Sabouraud′s dextrose agar with antibiotics was incubated at 25°C and brain hearth infusion broth at 37°C. A floccose growth was seen on Sabourauds dextrose agar in 3 days, and a fluffy mass in brain heart infusion broth in 5 days. Lactophenol cotton blue mount and slide cultures from these isolates confirmed our earlier findings. Since the specimen taken from the right eye of the patient twice over a period of 3 weeks grew the same fungus, identified as Paecilomyces variotii by its morphological characteristics, the diagnosis was definitely anterior endophthalmitis caused by P. variotii following intraocular lens implantation. On the basis of these findings, intraocular instillation of corticosteroids and voriconazole was initiated. Currently, the patient is free from symptoms and the vision has improved. The identification of the isolate as P. variotii was also confirmed by Department of Microbiology (Mycology Division), Postgraduate Institute of Medical Education and Research, Chandigarh. Discussion Post-operative infectious endophthalmitis can be encountered after any intraocular surgical procedure, fungi accounting for only 3% of the cases. [1] Fungal endophthalmitis occurring after a latent period of upto 210 days after surgery is known. [2] This is in agreement with about 120 day latency period seen in this case. Paecilomyces spp. are considered non-pathogenic saprophytes found in soil and decaying fruits and Vegetables. [1],[3] P. lilacinus and P. variotii are the most common species to cause human infection. [2],[4] The majority of published case reports involving P. lilacinus among healthy uncompromised host are of endophthalmitis that occurred following intraocular lens implantation. [5] The colour of the colony, and certain microscopic features help in the speciation. [1],[2],[6] Another feature that helps in species identification is thermophilicity. [6] P. crustaceus and P. variotii are thermophilic and can grow well at temperatures as high as 50°C and possibly 60°C. [6] The colonies are flat, powdery, or velvety in texture; colour is initially white and becomes yellow, yellowish green, yellowish brown, olive-brown, pink, or violet depending on the species. [1],[2],[3],[4],[6] Through microscopy septate hyaline hyphae, conidiophores, phialides, conidia and chlamydospores are observed. Conidiophores are often branched and carry the phialides at their tips. The phialides are swollen at their bases and taper towards their apices. They are usually grouped in pairs or brush like clusters. Conidia are unicellular, hyaline to darkly coloured, smooth or rough, oval to fusoid and form long chains. Chlamydospores are occasionally present. [1],[2],[3],[4],[6] Colonies of P. variotii are fast growing, powdery to suede-like, funiculose or tufted, and yellowish brown or sand coloured. Conidiophores bearing dense verticillately arranged branches bearing phialides. Phialides are cylindrical or ellipsoidal, tapering abruptly into a rather long and cylindrical neck. Conidia are subspherical, ellipsoidal to fussiform, hyaline to yellow, smooth walled, 3-5 x 2-4 μm and are produced in long divergent chains. Chlamydospores are usually present, singly or in short chains, brown, subspherical to pyriform, 4-8 μm in diameter, thick walled to slightly verrucose.[4] Since the specimen taken from the right eye of the patient twice over a period of 3 weeks grew the same fungus, identified as P. variotii by us and the reference laboratory, the diagnosis is definitely anterior endophthalmitis caused by P. variotii following cataract surgery with intraocular lens implantation [Figure - 1],[Figure - 2],[Figure - 3],[Figure - 4].[10] References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10076f4.jpg] [mb10076f1.jpg] [mb10076f3.jpg] [mb10076f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}