 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
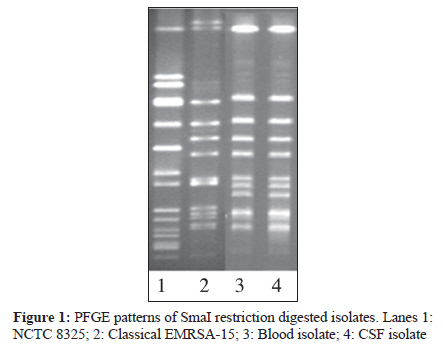
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 255-257 Case Report A variant epidemic methicillin resistant Staphylococcus aureus-15 cavernous sinus thrombosis and meningitis: A rare occurrence with unusual presentation HB Veena Kumari1, D Nagaraja2, S Nagarathna1, GB Kulkarni2, CS Praveen1, S Nadig3, G Arakere3 1 Department of Hospital Infection Surveillance System, Neuromicrobiology, Bengaluru-560029, India Keywords: Cavernous sinus thrombosis, EMRSA-15 variant, meningitis Introduction CST is a rare clinical entity with high morbidity and mortality. S aureus meningitis accounts for 2%-10% of cases of bacterial meningitis. Over 50% of such cases are nosocomial, while the remaining are community-acquired. In recent times, hospital-acquired central nervous system infections are attributed to methicillin resistant S aureus (MRSA), and community-acquired MRSA (CA-MRSA) strains as major community pathogens are also being introduced into the healthcare system. The clinical situations that predispose to the development of CST and meningitis are neurosurgical intervention, contiguous infection, and bacteraemia. Sinusitis (sphenoid and ethmoid) seems to be the most common primary source of CST and also one of the origins of infection in S aureus meningitis. [1],[2],[3],[4] EMRSA-15 and EMRSA-16, the pandemic clones of MRSA, have become the predominant hospital-associated MRSA in UK. [5] EMRSA-15 has been detected in many countries and characterized as belonging to SCCmec type IV and ST 22; these cases are mainly associated with hospitals. We report a case of rare occurrence of EMRSA-15 CST with meningitis. Case Report A 15-year-old boy presented to the emergency department with history of constant bifrontal headache for 7 days, intermittent fever with vomiting for 4 days, swelling of the right eye followed by swelling of the left eye, and altered sensorium for 2 days. There was no history of seizures, head injury, skin or soft-tissue infections, diabetes mellitus, or any immunodeficient state, but he had history of recurrent upper respiratory tract infections. On examination, he was febrile (103° F) with pulse rate of 140 /minute, blood pressure of 110/70 mmHg, and respiratory rate of 28/minute. Neurologically, he was in altered sensorium, with no response to commands. There was bilateral proptosis, ptosis, and chemosis of the eyes (right>left), with absent doll′s eye movements; both pupils were dilated and not reactiing to light. Papilloedema was present. There was paucity of movements on the left side, with bilateral brisk deep tendon reflexes and extensor plantar response. In addition, he had neck stiffness and Kernig sign was positive. A clinical diagnosis of CST with meningitis and cerebritis/ arteritis was considered. Computed tomographic (CT) scan of the brain showed enhancement of the cavernous sinuses, with prominent bilateral superior ophthalmic veins and opacity and fluid collection in the ethmoidal and sphenoidal sinuses. Magnetic resonance imaging (MRI) showed pan-sinusitis, with diffuse enhancement and cerebritis in the right frontotemporal region. With the imaging studies showing pan-sinusitis, contiguous spread of the infection from the sinuses to the intracranial compartment was considered. Blood culture was done and lumbar puncture (LP) performed. The patient′s blood sugar was normal and HIV status was negative. The transthoracic echocardiogram was normal. Surgical drainage of the paranasal sinuses was not performed due to the poor general condition of the patient. The patient was started on recommended doses of intravenous ceftriaxone, amikacin, and metronidazole. The cerebrospinal fluid (CSF) was turbid, with polymorphonuclear pleocytosis of 1400 cells/mm 3 . protein and glucose were 249 mg/dl and 39 mg/dl, respectively. Gram′s stain showed no evidence of bacteria. Both CSF and blood cultures showed growth of S aureus, and this was confirmed using standard tests like catalase, slide and tube coagulase, and growth on mannitol salt agar. Screening for methicillin resistance by cefoxitin (30μg) disc diffusion test was done as per standard guidelines. Zone diameters were recorded as recommended by CLSI and the isolates identified as MRSA. Antibiotic susceptibility testing was performed by Kirby-Bauer disc diffusion method and both isolates were found to be resistant to gentamicin, erythromycin, and ofloxacin, while being sensitive to tetracycline, ciprofloxacin, clindamycin, linezolid, and vancomycin. Treatment was revised to include intravenous vancomycin and oral rifampicin in recommended doses, along with other supportive treatment. The patient started showing improvement after 5 days of the treatment, and the same was continued for 4 weeks. Screening of the nose, axillae, and groin was carried out before treatment as per the hospital protocol for MRSA screening, and all were negative for MRSA. CSF and blood cultures were sterile after a week′s treatment. The patient was discharged after 2 months of hospital stay. One year into the follow-up, he has residual right occulomotor nerve palsy, with mild left hemiparesis. The MRSA isolates from the blood and CSF were genotyped. Both isolates had type IV SCCmec cassette with type 2 cassette chromosome recombinase (ccr) AB and staphylococcal protein A (spa) type of t852. [6],[7],[8],[9] Pulsed-field gel electrophoresis (PFGE) patterns are shown in the [Figure - 1] and demonstrate identical patterns for blood and CSF isolates, which are related to classical EMRSA-15 and differ by 3-4 bands. Discussion Septic CST is a lethal illness associated with high mortality and morbidity. Sinusitis is the most common primary source. There have been increasing reports of serious diseases attributed to hospital-associated (HA) methicillin-resistant strains of S aureus (HA-MRSA) as well as CA-MRSA. [1],[2],[3] In this report, we describe a culture-proven case of CST meningitis that was caused by CA EMRSA-15, the primary site of infection probably being the sinuses; blood and CSF cultures were positive. Our search for the potential focus of infection identified a contiguous sinusitis, and this was supported by the MRI findings. The features of meningitis were complemented by the typical clinical manifestations of CST. We hypothesize that the patient may have had spread of infection from the contiguous sinuses, with seeding of the meninges and the cavernous sinus. Microbiological culture of the affected paranasal sinuses was not performed. This could have contributed to a definite diagnosis. The laboratory investigations and CSF findings were all consistent with the diagnosis of pyogenic bacterial meningitis. The negative Gram′s stain of the CSF is not unusual, as positive CSF Gram′s stain has been reported in only 20%-59% of cases of MRSA meningitis. [2] CA-MRSA differs from HA-MRSA in that the former is sensitive to multiple antibiotics, while the latter is typically sensitive only to vancomycin and linezolid. [10] The development of a serious infection in a young person without predisposing conditions is typical of CA-MRSA infection and this was seen in our patient too, though the antimicrobial resistance pattern is more consistent with a hospital acquisition. [3],[10] There has been a growing trend of antibiotic-resistant bacteria such as MRSA causing serious illness in the community. An increase in incidence of infections caused by CA-MRSA has been reported. [2] According to a recent review, there have been 11 published reports of CA-MRSA central nervous system disease in the last 4 years, the majority of them caused by USA 300, while one case was caused by EMRSA-16. There have been four CST cases with meningitis and brain abscess: three caused by USA 300 and one by ST93. [4] This is the first report from India of CST meningitis - itself a rare example of MRSA infection - which had a novel and serious presentation and was caused by a PVL-containing variant of EMRSA-15 isolate. Hospitals in the UK have experienced major problems with EMRSA-15 and the emergence of a variant with PVL is of serious concern in our country. As in our case, PVL-producing S aureus isolates are associated with greater possibility of disseminated infection. [4] Multilocus sequence typing (MLST) of three MRSA isolates from nasal swabs of healthy individuals with staphylococcal protein A(spa) type t852 belonged to ST 22 and similar PFGE patterns. EMRSA-15 variants, identical in PFGE patterns to this particular isolate, have also been isolated from nasal swabs of healthy people containing the same staphylococcal enterotoxins and PVL in Bengaluru on an earlier occasion (Gayathri, JMM -in press). Both isolates had similar staphylococcal enterotoxin patterns and were positive for PVL gene by PCR and amplified variant primers of hsdS1 region characteristic of ST22. [11] Records of 22 isolates of Spa type t852 from seven different countries are available but in none of the disease isolates. This case report should serve as a warning of the dissemination of EMRSA-15 into hospitals in and around Bengaluru, with the possibility of causing serious life-threatening diseases. Our experience with this case highlights the problems encountered in arriving at the correct diagnosis. Microbiological techniques can be vital, especially molecular characterization; it can assist in categorization of the strain as spontaneous or nosocomial and throw light on the distribution pattern and epidemiological profile. In our case, clinical investigation, radiological imaging, positive blood and CSF cultures, and molecular characterization aided in the diagnosis. According to the literature CA-MRSA has been isolated from CSF in only four out of seven cases of CA-MRSA CNS diseases. [4] Public health measures like notification, intensive laboratory surveillance, guidelines for healthcare professionals, and community education, if carried out religiously even in developing countries, can go a long way in containing the spread of CA-MRSA infections. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10077f1.jpg] |
| |||||||||
{kind=link}