 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
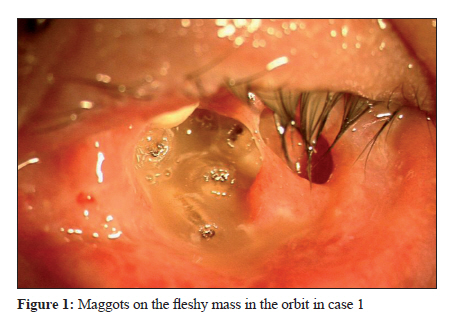
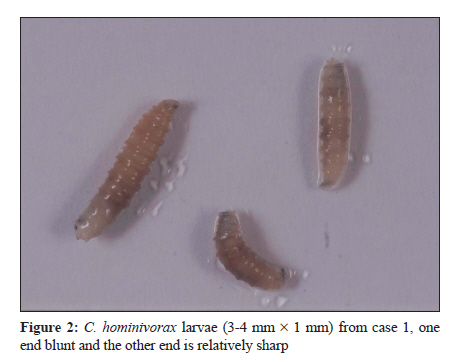
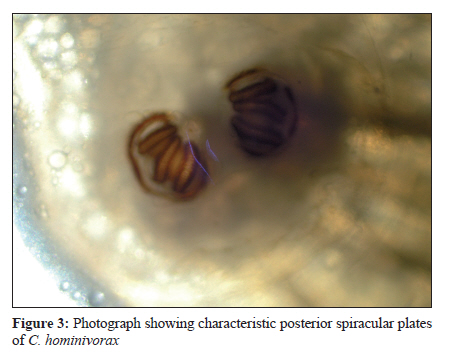
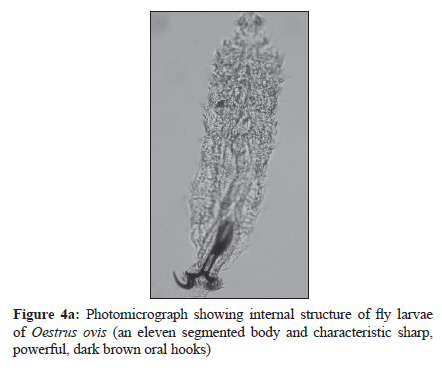
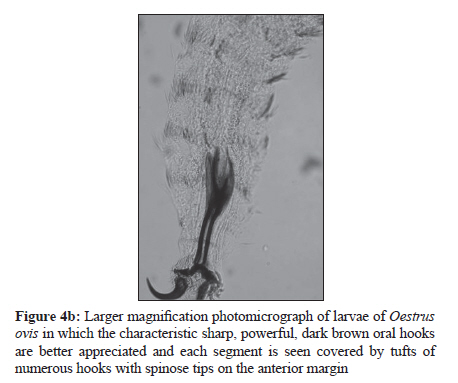
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 257-261 Case Report Ophthalmomyiasis: Three cases from North India S Khurana1, M Biswal1, HS Bhatti1, SS Pandav2, A Gupta2, SS Chatterjee3, WV Lyngdoh1, N Malla1 1 Department of Parasitology, PGIMER, Chandigarh-160 012, India Correspondence Address: Date of Submission: 30-Sep-2009 Code Number: mb10078 PMID: 20644320 DOI: 10.4103/0255-0857.66490 Abstract Three cases of external ophthalmomyiasis are reported here. The larvae were identified to be Oestrus ovis in two cases and Cochliomyia hominivorax in one. Two of the patients were immunocompetent while one was undergoing treatment for squamous cell carcinoma of eyelid. In the latter myiasis led to complete destruction of the eye.Keywords: Cochliomyia hominivorax, oestrus ovis, ophthalmomyiasis Introduction Myiasis is defined as the invasion of living and/or dead animal tissue by dipterous fly larvae (maggots) and is common throughout the tropics. [1] Occurrence and site of invasion of myiasis vary with the sanitary conditions, environmental factors, and presence of devitalised tissue that results from traumatic injury, erosive, ulcerative or haemorrhagic lesions. [1] Ocular involvement or ophthalmomyiasis is seen to occur in about 5% of all cases of myiasis. [2] Larvae, most commonly, attack the external surface of the eyes or ocular adnexia, e.g. the lids, conjunctiva or lacrimal ducts (external ophthalmomyiasis, EOM). In uncommon instances they may penetrate into the eyeball itself (internal ophthalmomyiasis, IOM) or may involve the orbit (orbital myiasis). EOM can usually be remedied without complications; however, IOM is very serious and often results in serious damage including blindness. Many dipterous flies of the genera Chrysomia (old world screwworm), Cochliomyia (New world screwworm), Oestrus (sheep botfly) and Hypoderma (cattle botfly) have been reported to cause myiasis in human and / or domestic animals. [1],[2],[3] EOM caused by dipterous fly larvae has been reported from India. [4],[5],[6],[7],[8] Most of these cases have been due to Oestrus ovis, and a few (mostly of orbital disease) due to Chrysomia.[5] We describe one case of orbital myiasis (Case-1) due to Cochliomyia hominivorax, and two cases of EOM caused by Oestrus ovis (Cases 2 and 3), who reported to our hospital during the last four years. Case Reports Case 1 An 80-year-old man from Panipat presented to the ophthalmology outpatient department (OPD) in 2005 with swelling of the right eyelid. The patient was a known case of squamous cell carcinoma of the eyelid skin, having undergone radiation therapy for the same four months ago. There was a re-growth at the same region of the tumour now. Examination revealed a fungating growth on his right eyelid. Ocular structures were completely damaged with total vision loss. A biopsy was taken and the wound was dressed. The patient was sent home with instructions to return after a week for appropriate therapy after receiving the biopsy report. The patient came a few days later with complaints of pain, discharge and a peculiar stench from the dressed area on the eye. On opening the dressing, it was noticed that there was a brown, fleshy, ulcerated, foul smelling mass all around the right orbit. There were a large number of maggots crawling over the fleshy mass [Figure - 1]. These were sent to department of Parasitology for identification. The specimen consisted of a white and shiny fly larvae measuring 3-4 mm x 1 mm. One end was blunt and the other sharp [Figure - 2]. Microscopically, the cuticle and hypodermis were also characteristic of fly larvae. The species was identified as larva of the fly C. hominivorax. The identifying features included deep constrictions between segments of the body and the characteristic configuration of anterior and posterior spiracles [Figure - 3]. The maggots, which were crawling over the surface of the mass, were removed manually. Orbit was irrigated with potassium permanganate solution to combat the foul smell. Sterile dressings were applied and systemic antibiotics were given along with analgesics. The patient failed to appear for follow-up following this visit. Case 2 A 30-year-old female resident of Chandigarh presented to the Ophthalmology-OPD, in 2008, with complaints of watering and foreign body sensation in right eye for two days. The patient belonged to middle socio-economic strata and had good personal hygiene. Visual acuity was 6/6 in both eyes, and mild conjunctivitis of the right eye was noted. On examination, two live larvae were recovered from the conjunctival sac and sent to the department of Parasitology for identification. Both the larvae measured 2 X 0.5 mm with characteristic sharp, dark brown oral hooks. Posterior spiracular plates were not seen as the larvae were probably immature. However, the body was divided into 11 segments, each being covered by tufts of numerous brown hooks with spinose tips on the anterior margin [Figure - 4a] and [Figure 4b]. The eleventh segment was bilobed, each lobe decorated with 12 hooklets. The larvae were thus identified as Oestrus ovis. Both the maggots were removed after applying topical anaesthetics and eye was washed with sterile normal saline. Topical antibiotic drops (ciprofloxacin) and steroid ointment were prescribed for daily use, and the patient asked to follow up regularly. When the patient returned the following day, the eye was clear of maggots. The patient was followed up for three weeks and no complication was recorded. Case 3 A 17-year-old female presented to the Ophthalmology-OPD in year 2009 with a history of watering of eyes and foreign body sensation in right eye for three hours. She resided in a colony in Chandigarh, where the rearing of sheep and goat is a common practice. She gave a history of some insect forcibly striking her eye. She called her sister for help who immediately noticed small insects crawling on the bulbar conjunctiva. The patient′s sister even managed to extract two of these insects. The girl attended the ophthalmology outpatient clinic, where conjunctival sacs of the right eye were seen to be full of insects (numbering more than 15). Some of them were crawling around freely while a few were embedded in the conjunctiva. Four of the maggots were stationed at the upper canthus, while the rest were seen in the lower cul-de-sac. Punctate scarring was seen in the conjunctiva. Visual acuity was 6/9 in the affected eye. The other eye was completely normal with vision of 6/6. The ophthalmologist, after applying a topical anaesthetic drop, removed the ′insects′ until none were seen under the slit lamp. Direct and indirect ophthalmoscopy showed no evidence of intraocular organisms or inflammation. The maggots were collected in normal saline and formal saline and sent to the department of Parasitology for further identification. The specimens were those of a fly larva measuring 1-2 mm X 0.3-0.5 mm and identified as larva of the fly Oestrus ovis, already described previously in Case 3. After removal of all the maggots, the eye was washed with sterile normal saline followed by application of topical antibiotic drops (tobramycin and moxifloxacin) and steroid ointment. When the patient returned the following day, the eye was clear of maggots, and visual acuity was 20/20. The patient was followed up for a further two weeks, and no complication was noted. Discussion Flies causing myiasis can be classified as either obligate or facultative. Obligate-myiasis producing species can complete their development only by parasitizing live hosts, whereas facultative species can develop on both living and dead organic matter. Primary facultative species initiate myiasis, whereas secondary species invade the host after primary or obligate species. Blowflies (Lucilia), screwworm (Chrysomia bezziana, Cochliomyia hominivorax) and flesh flies (Wohlfahrtia) cause obligate and / or facultative (e.g. Caliphoridae) myiasis of relatively short duration. Larvae mature within four to seven days, usually in wounds or body orifices. Bot flies (Oestridae or oestrids) are obligate parasites that are harboured within a host for several weeks to months. Today, even in the developing world, cases of human myiasis are relatively uncommon. In the West, such infections are a novelty, mostly occurring only in tourists returning from the tropics - predominantly Central, South America, and Africa. Although Oestrus ovis is by far the most common cause of EOM in man, [1],[3] fly species of genera Calliphora, Lucilla, Sarcophaga, Gastrophilus, Hypoderma, Musca, Callitroga, Cuterebra Dermatobia, Chrysomyia, Wohlfahrtia, Oedemagena, and Cochliomyia are known to cause ophthalmomyiasis in humans. [1],[2],[3] Sheep are the natural hosts for Oestrus ovis, and the fly is found in geographical areas where sheep are reared. [2] As such Oestrus ovis ophthalmomyiasis is worldwide in distribution; [2] however, in contrast, C. hominivorax ophthalmomyiasis was limited in distribution to America. Recently the agent is being reported more commonly east of the Atlantic. [9] Apart from location, exposure by way of occupation is also a risk factor. Shepherds are at greatest risk for Oestrus ovis infections and horse groomers are at risk for Gastrophilus spp. infection. [2] Poor living and hygiene conditions of patients may also contribute as a risk factor. [6] Patients with necrotising lesions in a setting of inadequate hygiene are susceptible to infestation by maggots. [2] The compromising of periorbital tissues by surgery, malignancy, ischemia, or infection predisposes the patient to myiasis. An interesting feature of Oestrus ovis is that it can deposit larvae while still in flight. The fly darts close to the eyes or nostrils and ejects a stream of larvae into the target area. [2] Three species of screwworms, Cochliomyia hominivorax (new world screwworm), Chrysomia bezziana (old world screwworm), and Wohlfahrtia magnifica (spotted flesh fly), cause overwhelming tissue destruction. [2] EOM is characterised by a condition similar to viral or allergic conjunctivitis, marked by pain, burning, itching, redness, and watering in the affected eyes. Often these symptoms are accompanied by the sensation of a foreign body moving in the eye. Many patients report having had an insect buzzing around their face or striking them in the eye immediately prior to the onset of symptoms. [1] The clinical features of OM are determined by the tissue invaded by the parasite. In EOM, maggots mainly infiltrate the conjunctiva and cornea causing conjunctivitis, and conjunctival haemorrhage; [1],[2] Conjunctivitis is characterized by irritation, lacrimation, pain, inflammation, and acute mucopurulent conjunctivitis from secondary bacterial infection. [1],[2],[6] Many fly larvae are armed with oral hooks, inter-segmental and caudal spines and a multi-layered spiny thoracic complex, which may cause direct mechanical damage and lead to haemorrhage, ulceration or even potential invasion, especially in neglected cases. [1],[2] Myiasis of the orbit is often associated with nose and sinus involvement. Severe tissue destruction is the rule. The most common invaders are Hypoderma bovis and Dermatobia hominis. [2] A serosanguinous discharge often exudes from infested wounds, and a distinct odour may be detected. Larvae that produce EOM can often be removed with forceps. Mostly, the larvae are readily visible on examining the eye. In some cases they can be seen travelling through the cornea. But sometimes, the diagnosis may require careful search; double eversion of the eyelid is often necessary to find maggots in the fornices. However, maggots are equipped with intersegmental spines and mouth claws that cling to tissue. For specific identification eggs, larvae, or flies should be placed in 70% alcohol and sent to a diagnostic laboratory equipped with personnel trained in entomological identification. In the laboratory, the larvae are fixed in hot formalin, dehydrated in ascending grades of alcohol, cleared in xylene and mounted in DPX to examine under high power for details which help in identification. [2],[3],[10] Because screwworm larvae penetrate deep into a wound, and other facultative larvae may exist more superficially in the same wound, specimens of larvae for laboratory diagnosis should be collected from the deepest part of the wound. Early growth stage larvae can often be carefully extracted from the eye with fine forceps. Care must be taken to prevent laceration of the larva; any portion of the larva remaining in the tissue cavity will produce an undesirable inflammatory response, or a bacterial infection. Anaesthetic drops may be useful to immobilize the larvae during removal. [2] Antibiotic ointments have also been used to help suffocate the larvae, thereby facilitating removal. Local antibiotics and topical corticosteroids further prevent secondary bacterial infection and reduce inflammation. [2] Follow-up examinations are advisable to rule out complications or the existence of additional larvae. Acknowledgments We thank Dr. Palash Samanta and Dr. Shivapriya (Senior Residents) for help in collection of the samples. References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10078f4a.jpg] [mb10078f1.jpg] [mb10078f4b.jpg] [mb10078f3.jpg] [mb10078f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}