 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
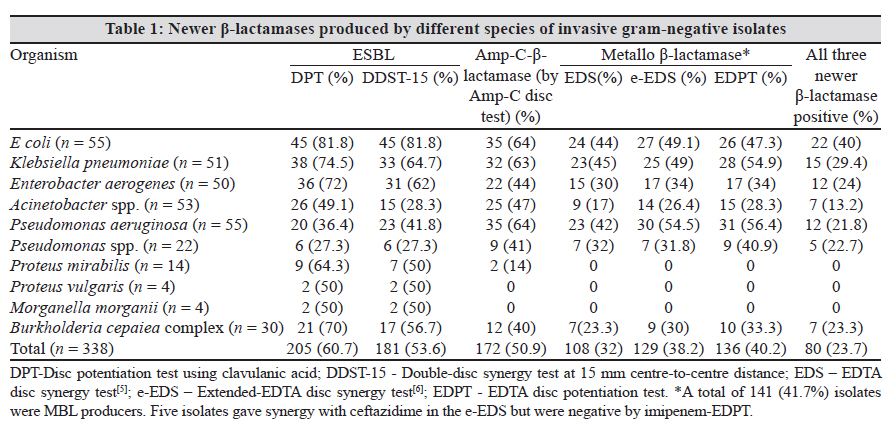
Indian Journal of Medical Microbiology, Vol. 28, No. 3, July-September, 2010, pp. 267-268 Correspondence High prevalence of co-expression of newer β-lactamases (ESBLs, Amp-C-β-lactamases, and metallo-β-lactamases) in gram-negative bacilli SS Chatterjee, R Karmacharya, SK Madhup, V Gautam, A Das, P Ray Department of Medical Microbiology, PGIMER, Chandigarh, India The newer β-lactamases, including extended-spectrum β-lactamases (ESBLs), Amp-C-β-lactamases, and metallo-β-lactamases (MBLs), have emerged worldwide as a cause of antimicrobial resistance in gram-negative bacteria (GNB). [1] Genes for all these three enzymes are often carried on plasmids, facilitating rapid spread between microorganisms. [1] The presence of ESBLs and Amp-C-β-lactamases in a single isolate reduces the effectiveness of the β-lactam-β-lactamase inhibitor combinations, while MBLs and Amp-C-β-lactamases confer resistance to carbapenems. Often these enzymes are co-expressed in the same isolate. We conducted this study to detect all three of these newer β-lactamases in GNB. ESBL, Amp-C, and MBL production were determined in 338 GNB isolates [Escherichia coli (55), Kliebsella pneumoniae (51), Enterobacter aerogenes (50), Acinetobacter calcoaceticus-baumannii complex (53), Pseudomonas aeruginosa (55), Pseudomonas spp. (22), Proteus mirabilis (14), Proteus vulgaris (4), Morganella morganii (4), and Burkholderia cepacia complex (BCC) (30)] from invasive sites (blood, cerebrospinal fluid, sterile body fluids, pus, broncho-alveolar lavage (BAL), and tissue). ESBL production was tested by two methods: the CLSI disc potentiation test (DPT), [2] and the double-disc synergy test (DDST). [3] Five different cephalosporins [cefotaxime (30 μg), ceftazidime (30 μg), aztreonam (30 μg), cefoperazone (75 μg), and cefepime (30 μg)] were used in the CLSI DPT test. [2] DDST was performed against cefotaxime (30 μg), ceftazidime (30 μg), aztreonam (30 μg), and cefepime (30 μg) at distances of 15 mm (centre-to-centre, DDST-15), 20 mm (DDST-20), and 25 mm (DDST-25) from a clavulanic acid (10 μg) disc. [3] Detection of Amp-C-β-lactamases was done by the Amp-C disc test,[4] while MBL production was tested by three methods: EDTA-disc synergy test (EDS), [5],[6] extended-EDTA disc synergy test (e-EDS), [6] and EDTA disc potentiation test (EDPT). [5] All MBL-positive isolates were tested for substrate profiles by EDPT against meropenem and ceftazidime. All isolates were tested for in vitro susceptibility against gentamicin (10 μg), amikacin (30 μg), and ciprofloxacin (5 μμg), following CLSI guidelines. [2] The order of sensitivity in the detection of ESBLs was: CLSI-DPT (205, 60.7%), DDST-15 (181, 53.8%), DDST-20 (111, 32.8%), and lastly DDST-25 (65, 19.2%). However, three P aeruginosa isolates were DDST-15 positive while being CLSI-DPT negative [Table - 1]. The order of activity against substrates for ESBLs was: cefotaxime (88.8%), cefoperazone (86.8%), ceftazidime (85.9%), cefepime (65.9%), and aztreonam (61.5%). One hundred and seventy-two (50.9%) isolates were found to be Amp-C-β-lactamase producers [Table - 1]. MBL detection using EDPT (136, 40.2%) and e-EDS (129, 38.2%) was more sensitive than EDS (108, 32%) [Table - 1]. Five isolates that were negative by imipenem-EDPT gave synergy with ceftazidime alone in the e-EDS as well as in the ceftazidime-EDPT; thus, 141 (41.7%) isolates were MBL producers. Order of activity against substrates for MBLs was: imipenem (96.5%), meropenem (41.8%), and ceftazidime (36%). Interestingly, 43 (30.5%) (E coli - 18, K pneumonia - 8, E aerogenes - 8, P aeruginosa - 6, Pseudomonas spp. - 3) of the 141 MBL producers were sensitive to both imipenem and meropenem by the CLSI DDST, with zone sizes of 16-21 mm. Of the 338 isolates, 80 (23.7%) produced all three of the newer β-lactamases [Table - 1]. In vitro resistance to amikacin, gentamicin, and ciprofloxacin was significantly higher (P < .05) in isolates producing all three newer β-lactamases compared to the rest (68.5%, 97.3%, and 83.6% vs 50.8%, 59.8% ,and 52.5%, respectively). References
Copyright 2010 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb10083t1.jpg] |
| |||||||||

{kind=link}