 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
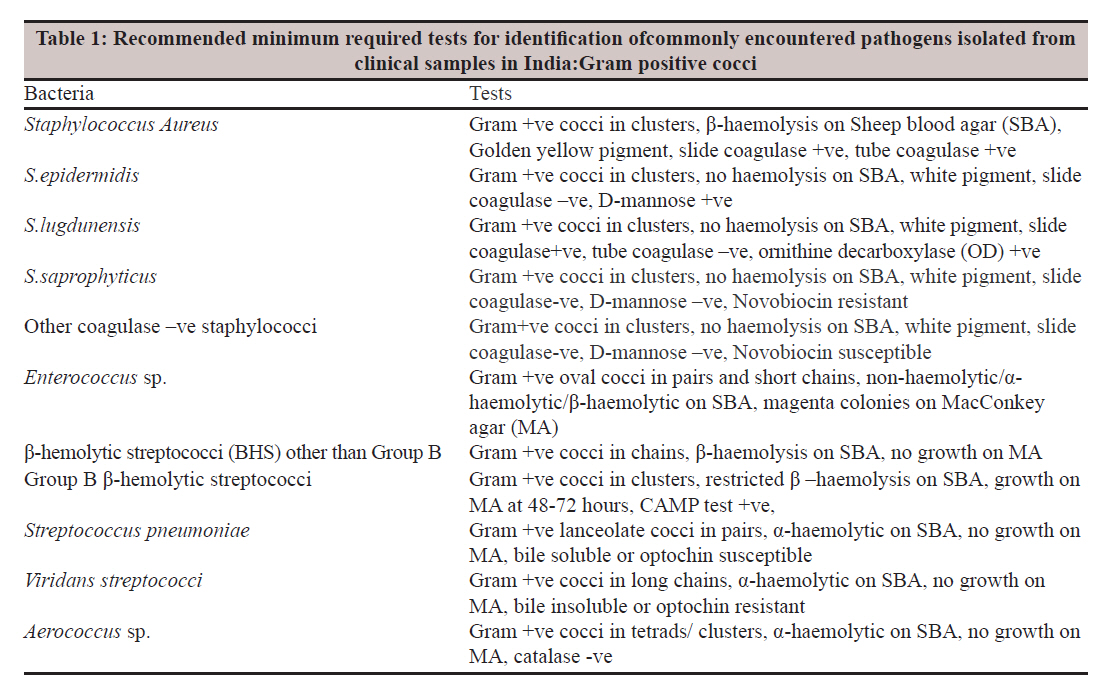
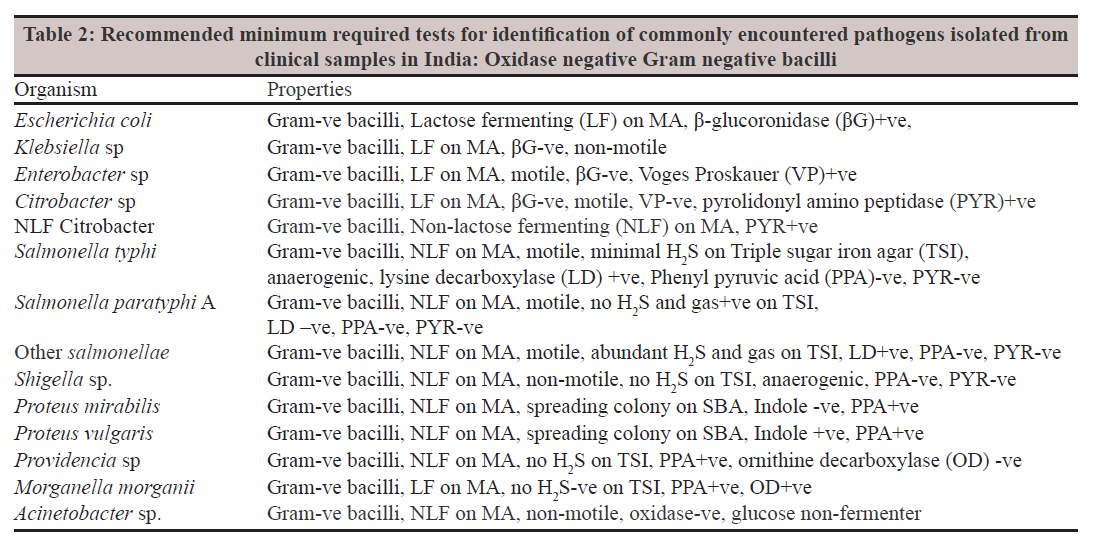
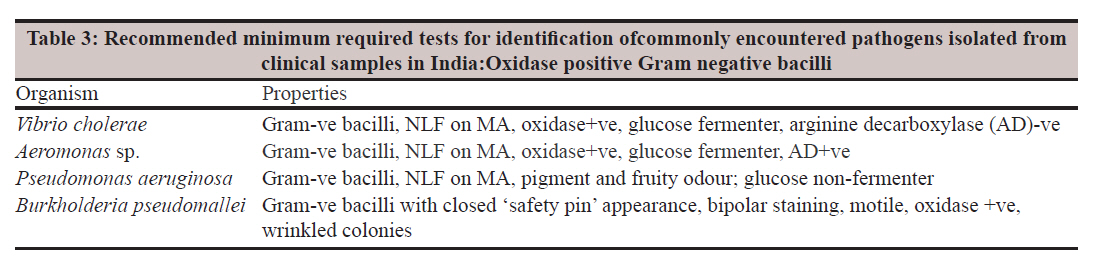
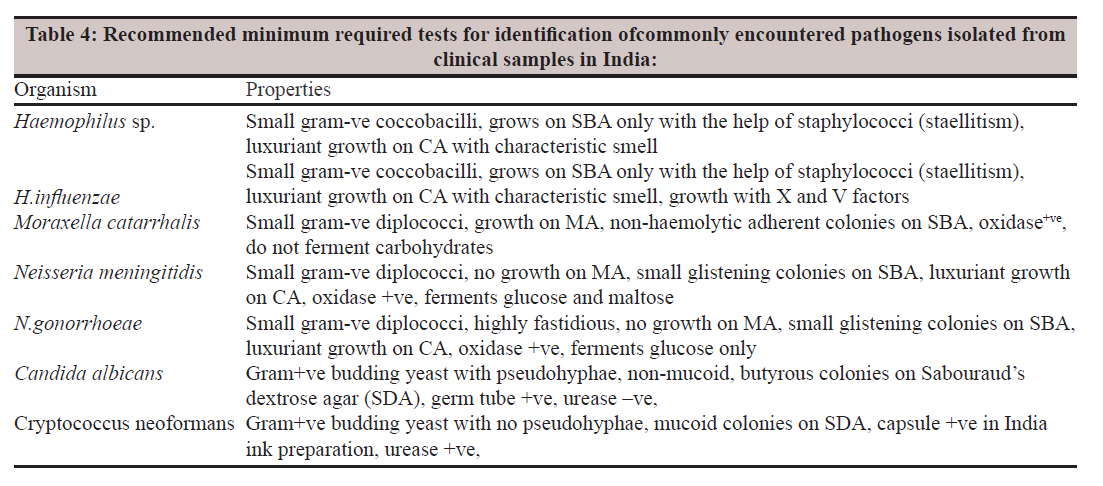
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 336-340 Review Article Bacterial identification in the diagnostic laboratory: How much is enough? BN Kootallur, CP Thangavelu, M Mani Dr. Brahmadathan Kootallur, Microbiological Laboratory, 12A Cowley Brown Road (East), R.S. Puram, Coimbatore - 641 002, India Date of Submission: 21-Jan-2011 Code Number: mb11085 PMID: 22120791 Abstract The major impetus for bacterial identification came after the advent of solid culture media. Morphological appearance of bacterial colonies was often sufficient for their identification in the laboratory. Even in modern times, preliminary identification of most cultivable bacteria is based on such morphological characters. Advances have been made media for the presumptive identifi cation of common organisms encountered in clinical samples. Phenotypic characterisation of bacteria with, physiological tests with a battery of biochemical tests differentiate related bacterial genera as well as confirm their identity. . Each laboratory can select its own method(s) of identification, provided they are based on scientific / epidemiological evidence; clinical laboratory and standards institute (CLSI) is a widely accepted organization and laboratories in many parts of the world follow its recommendations for bacterial identification. Some of the latest advances in identification include Matrix Assisted Laser Desorption Ionization - Time of Flight Mass Spectroscopy (MALDI-TOF) is a state of art facility used for fast and reliable species-specific identification of bacteria including Mycobacteria and fungi including yeasts. However the single most important factor that decides the method of bacterial identification in any laboratory is the cost involved. In the final analysis, selection of tests for bacterial identification should be based on their standardization with proper scientific basis. Considering the cost and lack of easy availability of commercial kits, we have put forward a simplified and rapid method of identification for most commonly encountered bacterial pathogens causing human infection in India Keywords: Bacterial identification, indian format, rapid tests Introduction Bacterial identification and determination of its antimicrobial susceptibility pattern is the cornerstone of clinical microbiology. [1] Growth requirements, colony characters on standardised culture media and a variety of biochemical and serologic characters help in the identification of bacteria up to genus and species level. This forms the basis for Koch-Henle postulates (Koch′s postulates in short). [2] In modern times, this has helped to generate data on host-parasite interactions, therapeutic decisions and epidemiologic investigations. Modern molecular techniques have gone several steps ahead and have added to the armamentarium of tests. [3],[4],[5] In resource crunch situations, laboratories often restrict themselves in this process of identification. The often raised query is: Is it really necessary to identify a "coliform bacilli" as Escherichia coli or Klebsiella sp. when one knows for sure that it is the agent that is causing infection in the patient. It is argued that the more important point is to determine its antibiotic profile so that appropriate therapy can be initiated at the earliest possible time. On the other hand, routine bacterial identification gives valuable epidemiologic information which in many situations can help in formulating appropriate antibiotic policy or even preventive measures. With newer pathogens emerging and older ones reemerging, identification of the agent becomes crucial in instituting such measures. This raises an important question on bacterial identification: How much is enough? Methods of Bacterial Identification The major impetus for bacterial identification came after the advent of solid culture media. [6] Morphological appearance of bacterial colonies was often sufficient for their identification in the laboratory. In fact, this was the one of the significant points towards the establishment of Koch′s postulates. Even in modern times, preliminary identification of most cultivable bacteria is based on such morphological characters. Many laboratories have started using chromogenic agar media for the presumptive identification of common gram negative bacilli encountered in clinical samples. [7] With phenotypic characterisation of bacteria done towards their systematic classification, physiological tests became the method of their identification. In countries like India, such tests continue to be the preferred method of laboratory identification. A battery of biochemical tests that will differentiate related bacterial genera as well as confirm their identity are readily available in the market to suit different grades of laboratories. Occasionally, few laboratories standardise their own battery of tests to make it cost effective and convenient for use. [8] In certain situations, such tests have become the bench mark for other laboratories in India. [9] This is true of teaching hospitals/institutions where often detailed characterisation of bacterial species is undertaken for teaching/research purposes. Manual miniaturised or computational system of identification became a major innovation in the 1960′s that became a forerunner of automated systems for the future. [1],[10] This never really picked up as a preferred method in Indian laboratories because of the cost factor. Introduction of a combined system of identification and susceptibility testing in 1978 laid the foundation for automation in clinical microbiological laboratories that came in 1983. [10] Although such systems could reduce the turn over time to two to four hours, they too did not pick up in the Indian laboratories because of the heavy capital and recurring cost. A more rational and easily available method was the DNA amplification method/s which saw wide application in many Indian laboratories. [mb11],[12],[13] In turn, wide acceptance led to decreased cost and the cycle continues to generate modification of techniques to suit variety of pathogens. Such techniques also have the advantage of identifying the pathogen/s directly from the clinical sample. Bacterial identification and evidence based clinical microbiology The concept of evidence based health practices came up in response to diagnosis and prognosis of disease through research and dissemination of new knowledge that can meet high standards of critical review. [14] Although evidence based treatment is well established, the role of evidence based diagnosis is less defined. This is probably because the advances in technology have led to higher cost of diagnosis which has a negative effect in research and diagnosis in resource crunch situations. Newer techniques of bacterial identification are costly and therefore old techniques continue to hold fort in most diagnostic laboratories in India. Thus, evidence based microbiology has not kept up with the expectations of patients and physicians alike. As stated at the outset, the often repeated question is: How does identification of a bacterial agent help in the diagnosis and treatment? It is true that an unidentified "coliform bacilli" recovered from a mid stream urine sample of a patient with an uncomplicated significant bacteriuria is as good as an agent identified as say, Escherichia coli. This holds true in acute infections when the bacterial agent is grown in pure culture or in significant numbers. A similar situation also exists when the agent is recovered from an otherwise sterile body site. But the problem arises when the agent is recovered along with a mixture of normal saprophytic flora; the agent needs to be fully identified so as to differentiate it from the normal flora with which it may resemble in many aspects. In special situations, an otherwise saprophytic organism such as Staphylococcus epidermidis can also act as a pathogen where identification is the first step in establishing its pathogenic role. [15],[16] This creates two scenarios. One in which minimal identification with one or two characters is sufficient for bacterial identification and another one in which a battery of tests is required to identify or even characterise the bacterial isolate. In either case, these characters have to be listed in detail for each bacterial species in a style that suits standard operating procedures (SOP). The list should also mention clinical specimen from which each of these bacterial species is recovered. It may not be possible at this point in time to have a uniform set of identification protocols for the whole country; but nonetheless, each laboratory can document its protocols in such a way that it can be a trend setter of sorts for future course of action. This is what exactly the National Accreditation Board for Laboratories (NABL) recommends. Each laboratory can select its own method/s of identification, provided they are based on scientific/ epidemiological evidence; but they should be documented thoroughly and with no ambiguity. NABL does not recommend any specific reagent, media, or biochemical tests; but maintaining and adhering to the SOP is mandatory for accreditation. This ensures certain quality to laboratories despite varying laboratory standards. Teaching Hospitals Versus Commercial Diagnostic Services Where do commercial diagnostic centres stand as against teaching hospitals in this regard? An accredited diagnostic service facility should stress predominantly on high quality and good turnaround time to satisfy the needs of its customers. On the other hand, a good teaching hospital laboratory will stress on both patient services and teaching programs and therefore their protocols will include more detailed characterisation of various bacterial species. This often may end up in protocols that are much more stretched out than are really necessary for the identification of the organism. As stated earlier, these differences should not make a great difference, as long as the SOPs are well written and strictly adhered to. The Clinical Laboratory and Standards Institute effect Clinical Laboratory and Standards Institute (CLSI, previously NCCLS) has recently published an abbreviated identification system (Approved Guidelines, 2 nd Edition) for the laboratory identification of diverse pathogenic bacteria and yeasts. [17] This includes both cultural and biochemical characters well suited for small and medium bacteriologic laboratories. This is a document developed through a consensus process that describes criteria for operating practice, procedure, or material for voluntary use. These tests allow reliable identification of organisms with a high degree of certainty, decreasing the necessity for time consuming tests. This, CLSI says, enhances timely patient care. CLSI is a widely accepted organisation and laboratories in many parts of the world follow its recommendations for bacterial identification. The tests described in the document include tests/characters that have been validated by workers in the US. Expertise as a microbiologist and initial correctness in the interpretation of Gram stain and colony characters is essential for good results. Newer techniques The rapid advances in technology in the last few years have brought in some welcome changes in bacterial identification. One of the most promising technologies being used in many diagnostic laboratories is the Matrix Assisted Laser Desorption Ionization - Time of Flight Mass Spectroscopy (MALDI-TOF). This detects the protein profiles of bacteria based on the mass and electric charges of bacterial surface proteins. The capital cost of the equipment is high; but the consumable cost per test is only a few rupees. Moreover, the identification takes only a few minutes, compared to the few hours or even days by the conventional methods. Recent reports confirm the utility of this method in the diagnostic laboratory. [18],[19],[20] The GeneXpert(R) Mycobacterium tuberculosis/rifampicin (MTB/RIF) assay is a hand-free, on-demand, rapid and near-patient system that can simultaneously identify Mycobacterium tuberculosis and rifampicin resistance. [21],[22] It combines on-board sample preparation with real-time polymerase chain reaction (PCR) amplification and detection functions for nucleic acid analysis. It can deliver an accurate diagnosis of tuberculosis from sputum and other samples in less than two hours. The Cost Factor The single most important factor that decides the method of bacterial identification in any laboratory is the cost involved. Commercial kits consisting of multi-test systems never really picked up in the Indian market due to their prohibitive cost. A test with minimal cost and maximum specificity will always be more acceptable than a battery of tests that will cost more. In such a situation, the result will stop with a "coliform bacilli" rather than an Escherichia coli or Klebsiella pneumoniae. Past experience has shown that development of local reagents or locally standardised battery of tests with proper validation will attract a lot of attention. [7],[8] Other laboratories are then likely to standardise these tests to suit their needs as the cost factor would be handy and comfortable to handle. As more and more laboratories in the country follow suit, these tests are likely to become a national bench mark for identification. This in turn can subsequently become a national guideline for approved identification system. An Indian Format for Bacterial Identification Considering the cost and lack of easy availability of commercial kits, we have put forward a simplified and rapid method of identification for most commonly encountered bacterial pathogens causing human infection in India [Table - 1],[Table - 2],[Table - 3],[Table - 4]. For this, we have followed the CLSI document. [17] All tests for identification are rapid (2-4 hours) except for triple sugar iron agar, Christie, Atkinson, MunchPeterson (CAMP) test and novobiocin susceptibility tests. Our emphasis is on easy identification using minimal tests so that the system is within easy access of small and medium laboratories. We feel that under normal circumstances, speciation is not necessary for treatment (except for Salmonella sp.); this is also the CLSI recommendation. Further characterisation, if desired, can be undertaken using standardised methods. [22] Conclusions In the final analysis, selection of tests for bacterial identification should be based on their standardisation with proper scientific basis. How far one should go towards this should be decided by the quantum and nature of work, ability to standardise the tests and the cost factor. Maintenance of quality of tests, their interpretation and the documentation of results should be the basic objective on which the result is reported. Bacterial identification should be aimed to help the clinician to make a correct and rapid diagnosis as well as generate reliable data for future clinical, therapeutic and epidemiologic use. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11085t3.jpg] [mb11085t4.jpg] [mb11085t2.jpg] [mb11085t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}