 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
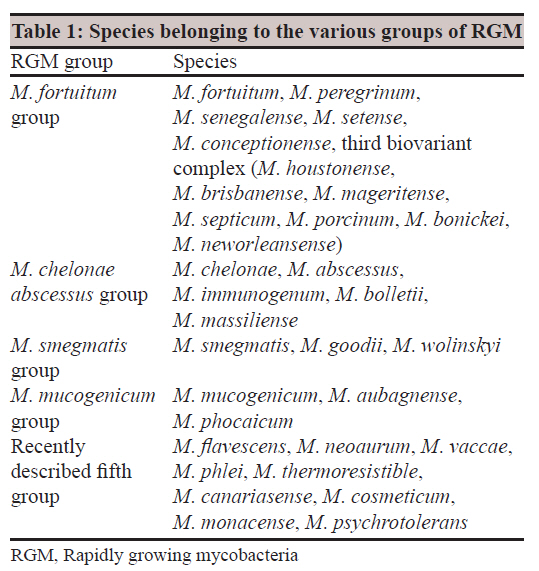
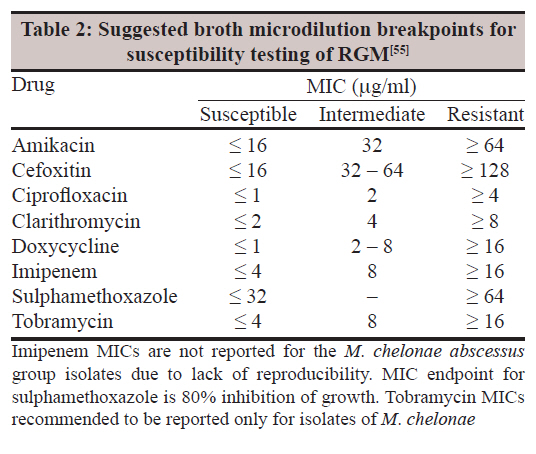
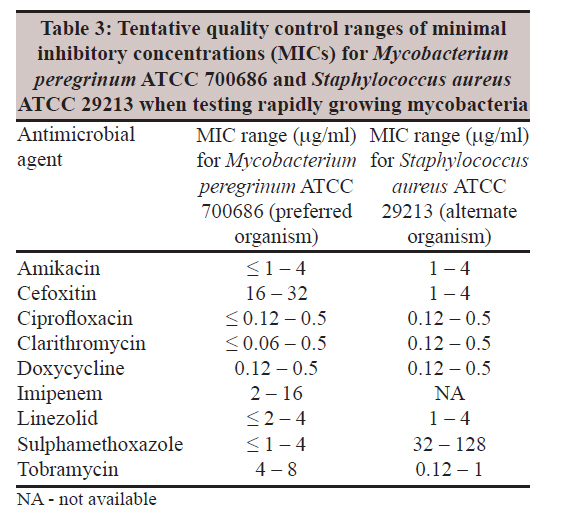
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 343-352 Review Article Laboratory aspects of clinically significant rapidly growing mycobacteria R Set, J Shastri Department of Microbiology, Topiwala National Medical College, Mumbai 400 008, India Date of Submission: 22-Apr-2011 Code Number: mb11086 PMID: 22120792 Abstract The pathogenic potential of the rapidly growing mycobacteria (RGM) has started being recognized. This is due to more sensitive and specific techniques in the laboratory. The RGM are generally defined as nontuberculous species of mycobacteria that show visible growth on agar media within 7 days. RGM are widely distributed in nature and have been isolated from natural water, tap water, and soil. Several biochemical tests, high performance liquid chromatography, and molecular techniques have been developed for rapid identification of these species. The American Thoracic Society and the Infectious Disease Society of America recommend that RGM should be identified to the species level using a recognized acceptable methodology such as polymerase chain reaction restriction enzyme analysis or biochemical testing and routine susceptibility testing of RGM should include amikacin, imipenem, doxycycline, the fluorinated quinolones, a sulphonamide or trimethoprim-sulphamethoxazole, cefoxitin, clarithromycin, linezolid, and tobramycin. The diseases caused by these organisms have varied manifestations. They have been responsible for a number of healthcare-associated outbreaks and pseudo-outbreaks. For recognition of outbreaks, it is important to be familiar with the causative organisms like RGM which are most frequently involved in healthcare-associated outbreaks and pseudo outbreaks. It is essential to intervene as soon as possible to interrupt this transmission. Large gaps still exist in our knowledge of RGM. Unquestionably more studies are required. Through this review, we wish to emphasize that reporting of RGM from clinical settings along with their sensitivity patterns is an absolute need of the hour. Keywords: Healthcare-associated infections, Mycobacterium fortuitum, Mycobacterium chelonae, Mycobacterium abscessus Introduction The increase in nontubercular mycobacterial (NTM) infections is a matter of serious public health concern. Amongst the NTM, rapidly growing mycobacteria (RGM) are emerging in previously unrecognized settings, with new clinical manifestations. RGM are widely distributed in nature and have been isolated from water and soil, tap water being the major reservoir. Many cases have been reported from India. Improvement in isolation and identification techniques has led to an increased awareness of the importance of RGM as human pathogens. The species of RGM which are common human pathogens have different virulence levels in diverse clinical settings and also have different drug susceptibility patterns. Hence an attempt has been made in this review to provide enough information about the clinical significance and the laboratory aspects of RGM. The RGM are generally defined as nontuberculous species of mycobacteria that show visible growth on solid laboratory media within 7 days. [1] The species of RGM capable of producing disease in humans consist of nonpigmented and pigmented species primarily belonging to the M. fortuitum group, the M. chelonae abscessus group and the M. smegmatis group. There are five groups each comprising a number of species which are shown in [Table - 1]. [1] Diseases caused by RGM include traumatic and surgical wound infections, skin and soft tissue infections, postinjection abscesses, central nervous system (CNS) disease, pulmonary infections, bone and joint disease, and catheter-associated infections. Predisposing host conditions are the immunocompromised state (steroids, HIV, and malignancy) and chronic lung disease (cystic fibrosis). Pseudo-outbreaks of disease, defined as clusters of false infections or artifactual clustering of real infections, have been associated with contaminated bronchoscopes and automated endoscope cleaning machines with tap water as the source of the organism. The M. fortuitum group accounts for the majority of the cases of localized cutaneous infections caused by RGM. Approximately 75% cases of disseminated cutaneous infections by RGM are due to M. chelonae and about 20% due to M. abscessus. The causative agent in most cases of pulmonary disease caused by RGM is M. abscessus. Rarely other RGM including M. chelonae, M. smegmatis, and M. fortuitum groups can be involved in pulmonary disease. Osteomyelitis after open fracture and secondary to puncture wounds is caused by the M. fortuitum group, M. goodii, and M. wolinskyi. The M. smegmatis group which was earlier considered as nonpathogenic is now known to cause both community acquired and healthcare-associated disease. Community acquired disease due to the M. smegmatis group is now known to involve post-traumatic cellulitis, localized abscesses, and osteomyelitis of a wound site. RGM infections in HIV-negative patients are mostly due to M. fortuitum and M. abscessus. Skin and soft tissue infections by direct inoculation, surgical wound infections, and catheter-related sepsis in HIV-negative patients are mostly caused by M. fortuitum. In patients who are HIV negative but are immunosuppressed due to steroid therapy or malignancy, disseminated infections are caused by M. chelonae. Clinical Significance The RGM are opportunistic pathogens that produce disease in a variety of clinical settings. The three most important species of RGM producing disease in humans are M. fortuitum, M. chelonae, and M. abscessus. NTM infections are usually not reported to public health department, thus data on incidence and species distribution are sparse. However, there have been suggestions that NTM disease is increasing. Amongst the NTM prevalence rates of RGM appear to be increasing. The prevalence of disease and the species responsible for causing it vary geographically. In some parts of Asia, RGM are a major cause of pulmonary NTM disease. This is in contrast to other parts of the world. In a surveillance study from the Netherlands, RGM caused only 3% of all pulmonary NTM infections and in United States it was 5%. In Asia RGM were generally found to cause 14% of pulmonary NTM infections but in three countries, i.e., India, Taiwan, and Korea this percentage rose to greater than 30% of pulmonary NTM infections. [2] A recent study in India showed that 36% of all NTM infections were RGM. This could reflect higher environmental exposure to RGM in Asia and also Asians may be more susceptible to RGM. This could also be attributed to better awareness and improved detection methods. This study also showed that RGM pulmonary infection due to M. abscessus and M. fortuitum are more common. In extrapulmonary, M. fortuitum and M. abscessus were mostly from postoperative laparoscopic skin and soft tissue infections. Postoperative mycobacterial abscess are usually due to M. fortuitum, M. chelonae, and M. abscessus. [3] Post-traumatic wound infections The most common infection seen with RGM is post-traumatic wound infection, the clinical picture of which varies from localized cellulitis or abscess to osteomyelitis. The M. fortuitum group are most commonly associated with skin and soft tissue infections usually following some type of penetrating injury. [4] Traumatic wound infection especially open fracture often involves the M. fortuitum third biovariant complex. In 1991, Wallace et al. characterized 85 isolates of unnamed M. fortuitum third biovariant complex all of which were disease associated. The majority of infections appeared 4-6 weeks following puncture wounds or open fractures. Stepping on a nail was the most frequently reported antecedent injury. [5] An unusual cutaneous infection with M. fortuitum has been reported from India. [6] The M. smegmatis group has been reported to be the causative agent in cases of infection following motor vehicle accidents with extensive cellulitis, soft tissue, and periosteal necrosis evident at the time of surgical debridement. M. wolinskyi and M. goodii have also been associated with post-traumatic wound infections. [7] We have also reported a case of subcutaneous abscess from our tertiary care centre in a patient of systemic lupus erythematosus. [8] An outbreak of furunculosis caused by M. fortuitum on the lower extremities was reported in patients who were patrons of a nail salon in California. [9] Other species including M. abscessus and M. mageritense have subsequently been recovered in other cases of furunculosis. Disseminated cutaneous infections M. chelonae is the most predominant organism in disseminated cutaneous infections caused by RGM and occurs when the host is chronically immunosuppressed. [10] Disseminated cutaneous disease with M. abscessus occurs rarely but is serious. Pulmonary The causative agent in the majority of chronic pulmonary disease caused by RGM is M. abscessus, underlying diseases being bronchiectasis, cystic fibrosis, [11] gastroesophageal disorders, and prior granulomatous disease such as sarcoidosis or tuberculosis. M. chelonae, M. smegmatis group, and M. fortuitum may rarely be involved in pulmonary disease. [12] M. fortuitum has been reported from cases of chronic aspiration disease secondary to underlying gastroesophageal disorders. In an Indian study, M. chelonae and M. fortuitum accounted for 67% of NTM from respiratory specimens. [13] M. immunogenum is able to grow in degraded metal working fluid and has been associated with hypersensitivity pneumonitis among metal grinders working in plants with contaminated metal working fluids. [14] M. thermoresistible has been reported from sputum culture of a patient with chronic pulmonary obstructive disease, diabetes, and purpura. [15] Among newly described RGM species causing pulmonary infections are M. phocaicum, M. aubagnense, M. bolletii, M. massiliense, M. goodii, and M. peregrinum. Healthcare-associated infections Healthcare-associated diseases with RGM are commonly due to M. fortuitum, M. chelonae, M. abscessus, and M. mucogenicum. The M. fortuitum group is responsible for the majority of cases of postsurgical wound infections caused by RGM. The most common isolate is M. fortuitum which is implicated in sternal wound infections, [16] and postinjection abscesses related to electromyography needles. [17] A case of injection site abscess due to M. fortuitum has been reported from India by Devi et al. [18] M. fortuitum has also been found from sporadic cases of surgical wound infections and catheter-related infections. A series of five cases of postsurgical wound infections in immunocompetent individuals who presented with delayed wound healing, discomfort over incision site, and chronic serous discharge have been reported from India. [19] The first case of human infection by M. senegalense was reported in a cancer patient in Korea. [20] M. peregrinum has also been found to be associated with surgical site infections. [21] A small number of cases have been published regarding wound infections following augmentation mammoplasty and cardiac surgery. [22],[23] Six clinical isolates of M. mageritense were recovered from sputum, bronchial wash, blood, sinus discharge, and two surgical wound infections from patients in Texas. [24] Sixty-seven clinical isolates of M. porcinum were obtained from wound infection, central catheter infections, and bacteraemia. [25] The most common pathogenic RGM recovered from central catheter associated infections is M. fortuitum. M. fortuitum bacteraemia in a patient of acute lymphoblastic leukemia with peripherally inserted vascular catheter has been reported from India. [26] M. septicum has also been recovered from catheter-related bacteraemia. [27] Reports regarding wound infection following laparoscopy have been published from India. [28],[29] The M. chelonae abscessus group has been involved in several healthcare-associated disease outbreaks including postcardiac surgery sternal wound infections and vein graft infections, plastic surgery, hemodialysis and wound infections following laparoscopy, liposuction, and post-tympanostomy tube placement. Also this group has been implicated in postinjection abscess outbreaks and healthcare-associated pseudo outbreaks associated with contaminated bronchoscopes, automated endoscope cleaning machines, and contaminated laboratory reagents. Healthcare-associated outbreaks involving the M. smegmatis group have included sporadic cases of catheter sepsis, infected pacemaker site, infections following cardiac and plastic surgery. Infections associated with surgical implants and a case of olecranon bursitis by M. goodii has been reported. [30] Bone and joint infections Osteomyelitis may follow open bone fractures, puncture wounds, and hematogenous spread from another focus. The most frequent pathogen recovered is the M. fortuitum group. M. fortuitum and M. chelonae dual infection following open fractures has been reported. [31] M. goodii and M. wolinskyi have also been associated with osteomyelitis. [7] Central nervous system disease CNS disease involving RGM is rare. Most of the reported cases have been associated with M. fortuitum. Two cases of ventriculoperitoneal shunt infection [32],[33] and a case of spinal tuberculosis have been reported from India. [34] Corneal infections A review of the literature from 1965 to 1992 regarding keratitis due to NTM revealed that the organism isolated in 55% cases was M. fortuitum and in 42% cases was M. chelonae abscessus group. Since early 1990 ocular infections due to RGM included cases occurring after keratoplasty and laser in situ keratomileusis (LASIK) surgery. [1] Several reports of keratitis by M. chelonae have been reported. M. fortuitum keratitis has been reported by Sanghvi. [35] An outbreak of keratitis by M. immunogenum has also been reported. [36] Cervical lymphadenitis Cervical lymphadenitis due to M. fortuitum has been reported in the literature. [37] Most of the patients had complete resolution or decrease in the size of the affected lymph nodes following therapy. Otitis media The most common RGM associated with chronic suppurative otitis media is M. abscessus. Also an outbreak by M. chelonae was reported in two ear, nose, throat clinics. [38] Laboratory Procedures Collection and transport of specimens Respiratory specimens The statement issued by American Thoracic Society (ATS) and Infectious Disease Society of America (IDSA) on diagnosis and treatment of infections caused by NTM emphasizes that evaluation of patients suspected of having pulmonary NTM infection should include the following: Chest radiograph; chest high resolution computed tomography (HRCT) scan if cavitation is absent on radiography; three or more sputum specimens for acid fast bacilli (AFB) analysis and exclusion of other disorders such as tuberculosis. [39] The chest radiograph in patients with RGM infections usually shows multilobar, patchy, reticulonodular, or mixed interstitial alveolar opacities with an upper lobe predominance. Cavitation is known to occur in 15% of cases. HRCT generally shows bronchiectasis and small nodules. If any such radiographic changes are seen, at least three sputum specimens should be submitted to the microbiology laboratory for AFB smear examination and mycobacterial culture. If sputum cannot be obtained, bronchoscopy with or without lung biopsy may be necessary. Tap water should be avoided while cleaning the bronchoscope. The patient should have at least two positive cultures from separate sputum specimens or at least one bronchial wash or lavage should yield RGM. Additional diagnostic criteria include transbronchial or other lung biopsy with mycobacterial histopathological features and positive cultures for RGM or biopsy showing mycobacterial histopathological features and one or more sputum or bronchial washings from which RGM is isolated. [40] Body fluids, pus and tissues Aseptic collection of body fluid or abscess pus by needle aspiration or surgical procedures is recommended. Swabs are not recommended for sample collection because they often have limited culture material and are also subject to drying which decreases the chances of growing the RGM. Culture and histopathological examination of tissue biopsies are the most sensitive ways of diagnosing infections due to RGM. Tissue biopsy specimen should not be wrapped in gauze or diluted in liquid material. If only a little amount of tissue is available, it may be immersed in a small amount of sterile normal saline (not formalin) to avoid excessive drying. [39] Blood Most RGM species grow well in routine blood culture systems. Collection of all specimens should be done by avoiding potential sources of contamination, e.g. tap water in which environmental mycobacteria are often present. Specimens should be collected in sterile, leak proof, appropriately labeled containers. Transport media and preservatives are not usually recommended. Refrigeration of specimens at 4 °C is preferred in case transportation is delayed by more than an hour. Specimens for mycobacterial analysis can be shipped with refrigerants such as cold packs. Antibiotics such as macrolides and quinolones should be limited during diagnostic evaluation of RGM diseases as these can decrease the yield of RGM. [39] Digestion and decontamination Digestion and decontamination procedures should be carried out on specimens collected from nonsterile body sites. The widely used method is the N-acetyl l-cysteine sodium hydroxide method. Decontamination for RGM has to be gentler than that for M. tuberculosis as they are more susceptible to decontamination. [39] Smear microscopy The recommended method for staining mycobacteria is the fluorochrome method. Ziehl Neelsen or Kinyoun stain is acceptable but less sensitive. It is more prudent to use a weaker decolorizing agent for staining RGM as they may be more sensitive to the AFB decolorization procedure. [39] Culture techniques All specimens for mycobacterial culture should be inoculated on both solid and liquid media. Broth cultures give higher yield of mycobacteria and produce rapid growth though the disadvantage is bacterial overgrowth. Solid media allow recognition of mixed mycobacterial infections, help us to observe colony morphology and growth rates, and serve as a backup when liquid cultures are contaminated. Recommended solid media are Lowenstein Jensen agar, Middlebrook 7H10, or 7H11 media. Cultures for RGM should be incubated at 28-30 °C. Some strains of M. chelonae may require between 28 °C and 33 °C. Optimal recovery of all species may require incubation at 28-30 °C and 35-37 °C. RGM grow within 7 days of inoculation. The time in days to the detection should be mentioned on the laboratory report as it can be helpful to clinicians to know that an RGM has been isolated. [39] RGM identification Species level identification is becoming clinically important, otherwise it is sometimes difficult to determine the clinical significance of the isolate. Therefore, identification of most RGM isolates to the species level and not merely as groups such as the M. chelonae abscessus group has been recommended. Biochemical identification Some of the biochemical tests commonly used for identification of the commonly encountered RGM species are three day arylsulfatase, iron uptake, nitrate reductase, tolerance to 5% NaCl, and utilization of the carbohydrates mannitol, inositol, and citrate. The utilization of carbohydrates has allowed more accurate identification of the commonly encountered species and discrimination of some not all newly described species. All members of the M. chelonae abscessus group and the M. fortuitum group show strong arylsulfatase activity at 3 days whereas the M. smegmatis group does not. The latter group is the only pigment producing group. Approximately 95% of M. smegmatis and 80% of M. goodii isolates develop a late yellow pigment after 7-10 days. High performance liquid chromatographic identification HPLC of mycobacterial cell wall mycolic acids is routinely used in many reference laboratories as a means of identifying isolates of NTM, but has been problematic with species of RGM. [41] Most studies show that HPLC is an acceptable method for separation of isolates of the M. fortuitum group and the M. smegmatis group from those of the M. chelonae abscessus group but cannot identify isolates accurately to the species level. It can be helpful for identification of RGM only when used in combination with other methods and under specifically standardized conditions. Thus identification of RGM based on HPLC alone is not sufficient. HPLC analysis of mycolic acids and partial gene sequencing for the first 500 bp 5'-end of the 16S rRNA gene has been used singularly and in combination to evaluate the final identification of RGM species. Consistent identification of all isolates differentiated to single species within the Mycobacterium genus was not possible by either method. Sequencing results often distinguished complexes containing fewer species and combining the results from each method increased the confidence of identifying the correct species. [42] Molecular identification Nucleic acid probes: The INNO LIPA multiplex probe assay (Innogenetics, Ghent, Belgium) utilizes the principle of reverse hybridization. [1] PCR amplification of the 16S 23S internal transcribed spacer (ITS) region yields biotinylated DNA which is hybridized with specific oligonucleotide probes immobilized as parallel lines on membrane strips. The addition of streptavidin labeled with alkaline phosphatase and a chromogenic substrate results in a purple brown precipitate on the hybridized lines. This single assay can identify a large variety of species without the need to select an appropriate probe. However, cross reactivity may be detected with strains of M. fortuitum and it fails to differentiate isolates of M. chelonae from that of M. abscessus. Two peptide nucleic acid (PNA) probes targeting 16S rRNA were developed to detect mycobacteria in positive broth cultures and for a routine use on AFB positive sputum smears. Fluorescence in situ hybridization (FISH) is an asset as no amplification equipment is required. However, NTM specific probe does not detect the presence of relatively common species like M. fortuitum, M. flavescens, and M. xenopi. All these species have more than one mismatch in the capture region of the NTM probe. [43] Amplified in situ hybridization with PNA probes for differentiation of Mycobacterium tuberculosis complex (MTC) and NTM on formalin fixed, paraffin-embedded archival biopsy and autopsy samples is also available. In one study on mycobacterial species identification in paraffin-embedded tissues, nested PCR was performed, and correlated with microbiological cultures. Twenty-five percent of 119 cases were found to be the M. fortuitum complex. [44] 16S ribosomal RNA (rRNA) gene sequence analysis: The 16S rRNA is an approximately 1500 nucleotide sequence encoded by the 16S ribosomal DNA. RGM except for M. chelonae and M. abscessus have two copies of the 16S rRNA operon. There are two hypervariable sequences known as regions A and B located on the 5Ͳ portion of the 16S rRNA of which hypervariable region A contains most of the species specific sequence variations in mycobacterial species and sequencing of this region allows taxonomic identification of most mycobacteria including RGM. A commercially available Microseq 500 16S ribosomal DNA (rDNA) bacterial sequencing kit (Applied Biosystems, Foster City, CA) based on PCR and sequencing of the first 500 bp of the bacterial rRNA gene has been evaluated and found to provide more rapid and more accurate characterization than do phenotypic methods. [45] Forty-seven isolates recovered in the L and T Microbiology Research Centre, Chennai, India were subjected to Microseq 500 and was found to allow recognition and reliable phylogenetic placement of species not described previously. [46] However one of the drawbacks of the system is failure to discriminate M. chelonae and M. abscessus, M. peregrinum, and M. septicum. A major limitation is that the database contains only one entry per species, the type strain and poses a problem with isolates that do not have an exact match in the database. Moreover, the Microseq 500 assay is expensive and hence may not be affordable in many clinical laboratories. Sequencing of the hsp65 gene: The gene for the 65 kDa heat shock protein (hsp65) exhibits greater interspecies and intraspecies polymorphism than the 16S rRNA gene sequence. Studies based on DNA sequencing have demonstrated interspecies allelic diversity within the RGM. Most sequencing has utilized a 441 bp sequence identified by Telenti known as the Telenti fragment. Detailed studies of several RGM including M. peregrinum, M. porcinum, M. senegalense, M. chelonae, and M. abscessus have shown four to six sequence variants per species that vary by two to six nucleotides within the 441 bp Telenti fragment. Unlike the 16S rRNA sequence analysis, the hsp65 sequence analysis can easily differentiate isolates of M. abscessus from those of M. chelonae. Sequences of the hsp65 gene allow even RGM species with a high degree of 16S rRNA gene similarity such as M. peregrinum, M. septicum, M. senegalense, M. fortuitum to be distinguished as distinct species. A limitation of hsp65 sequencing is that few or no sequences from more recently described RGM species are available in databases. Also detailed sequencing of older species having multiple strains is not available. [47] Polymerase chain reaction restriction enzyme analysis (PCR REA) of hsp65: Telenti et al. demonstrated that a portion of the hsp65 gene could be used for PCR REA and showed the patterns for some selected RGM. [48] Currently, this fragment is the most widely used sequence for PCR-based identification of the RGM and is highly accurate for the M. fortuitum group, the M. chelonae abscessus group, and the M. smegmatis group. It has not been studied for pigmented RGM. In one study all of 129 nonpigmented RGM could be identified using PCR REA. However, this system is not commercially available. In a study on molecular methods including genus and group-specific PCR and REA based on hsp65 gene for exact identification of M. fortuitum strains, REA was found to be a reliable and rapid approach to identify mycobacteria to the species level. [49] The advantages of REA are that the method of identification does not rely on the growth rate and nutritional requirements and the results of mycobacterial species can be generated rapidly. The disadvantages are that it requires knowledge of PCR and also requires extensive in house validation. PCR REA of 16S 23S rRNA sequence internal transcribed spacer: Extensive work has been done in India on the rapid identification of RGM by PCR REA targeting 16S 23S rRNA gene ITS. [50] This system is based on the amplification of approximately 1.8 kb fragment encoding the 16S 23S rRNA spacer region and flanking parts of both 16S and 23S rRNA gene. Restriction is carried out with three restriction endonucleases HhaI, HinfI, and RsaI to obtain distinct gene amplification restriction analysis patterns. This was found suitable for differentiating the species as M. fortuitum, M. chelonae, and M. smegmatis which showed distinct bands by all three restriction enzymes. Another ITS based system has been used in India only for the differentiation of M. chelonae complex. [51] Real time PCR: A 16S rDNA sequence based real time PCR assay has been developed and evaluated. With this assay more than 80% of the clinical isolates of NTM including M. fortuitum, M. chelonae abscessus group could be identified in a highly cost effective manner. [52] A multiplex real time PCR assay that can identify 93% of the pathogenic mycobacteria has also been evaluated. The primer targets included the 16S rRNA gene and the ITS. The sensitivity and specificity were each 99% or greater for the M. chelonae abscessus group and M. mucogenicum and 95% and 100%, respectively, for the M. fortuitum group. [53] DNA chip technology: This involves oligonucleotide array where molecular biology meets computer technology. It is designed to determine the specific nucleotide sequence diversity in mycobacterial species using DNA sequence of the rpoB and 16SrRNA genes followed by analysis of the oligonucleotide array hybridization pattern. In a study by Troesch et al., all isolates of M. chelonae, M. fortuitum, M. flavescens, and M. smegmatis were unambiguously identified by the DNA probe array. [54] To summarize various gene amplification techniques have been applied for rapid detection and identification of mycobacterial species. Among these PCR restriction analysis is preferred as they are simple and cost-effective. Gene amplification restriction assays targeting several genes like 16S rRNA, 23S rRNA, 16S-23S rRNA ITS, hsp65, rpoB have been developed. All these have been found to be easy and rapid in generating a restriction fragment length polymorphism (RFLP) pattern. However, the pattern becomes difficult to discriminate in the case of small size amplicons. Gene amplification assay using genus-specific primers targeting 16S 23S rRNA spacer region and flanking parts of 16S as well as 23S rRNA has been validated in reference strains and also on Indian clinical isolates from different parts of the country. This technique has been found to allow better and easier differentiation on gels as it targets a larger region and the fragments generated are bigger and can be easily separated and analyzed. In a recent study in India, NTM isolates have been speciated by amplifying a 360 base pair region of the rpoB gene and then subjecting the amplified products to reverse blot hybridization and restriction enzyme analysis. This technique has also helped in rapid and accurate identification of the isolates. [3] Susceptibility testing for RGM Most species of RGM have a unique drug susceptibility pattern which is important for therapeutic reasons. The four different methods used for susceptibility testing of RGM are broth microdilution, agar disc diffusion, agar disc elution, and the E-test. Broth microdilution: The CLSI (Clinical Laboratory Standards Institute) formerly known as NCCLS (National Committee for Clinical Laboratory Standards) has recommended the use of minimum inhibitory concentrations (MIC) determinations by using microbroth dilution as the gold standard for susceptibility testing of RGM. This is a MIC determination procedure with a series of concentrations of a number of drugs incorporated into a microtiter plate. The plates could be prepared in house by the user or commercially available plates from Trek Diagnostic Systems, Inc. (Columbia, OH) could be used. Results are available in 4-5 days. For isolates identified as RGM inclusion of the following 14 drugs is recommended: Amikacin, kanamycin, tobramycin, imipenem, doxycycline, clarithromycin, azithromycin, trimethoprim-sulphamethoxazole (TMP SMZ), amoxicillin-clavulanic acid, cefoxitin, ciprofloxacin, gatifloxacin, moxifloxacin, and linezolid. [55] The broth microdilution interpretive criteria for RGM has been shown in [Table - 2], along with the tentative quality control ranges of MICs for M. peregrinum ATCC 700686 and Staphylococcus aureus ATCC 29213 used when testing RGM in [Table - 3]. [55] Agar disc diffusion: This method applies the Kirby Bauer technique to the testing of RGM. This method has not been recommended for several years due to inherent technical problems. Therefore, therapeutic decisions should not be made on the basis of this method alone. Agar disc elution: This has been mostly used by laboratories where limited number of isolates are tested and that too only infrequently. This technique uses commercial susceptibility discs from which the drug is eluted into an oleic acid albumin dextrose medium and then mixed with melted agar to produce specific drug concentrations. E-test or gradient MIC test: This test combines the agar disc diffusion technique with an exponential gradient of antimicrobial dilutions to produce an MIC result. Interlaboratory studies by members of the Mycobacterial Subcommittee for Antimicrobial susceptibility testing of the CLSI have indicated that interpretation and reproducibility of the E-test MICs with RGM were often difficult. Molecular typing methods Molecular typing methods have become valuable tools in the investigations of outbreaks and pseudo outbreaks caused by RGM. Pulsed field gel electrophoresis: This is one of the most widely used methods for molecular strain typing of RGM. The technique consists of embedding the RGM isolates in agarose gel followed by lysing the DNA and digesting chromosomal DNA with specific restriction endonucleases. It is a time-consuming method as the RGM should be sufficiently grown in order to achieve proper results. However, PFGE is still the most common typing method for strain differentiation of RGM. [39] With some modifications of the original method, it is now possible to perform PFGE on almost all species of RGM. [56] Randomly amplified polymorphic DNA PCR analysis: This is a rapid and useful technique for the molecular analysis of pseudo outbreaks caused by RGM. In one study, the results obtained were very useful for characterization when the strains were characterized with at least three primers and all the isolates were processed together. [57] The discriminatory power of RAPD in comparison with PFGE has not been established. Management Medical treatment for RGM should be based on sensitivity profiles. Such studies are very limited in India. In the United States antimicrobial sensitivity patterns have been studied extensively over the years based on which the ATS has stated some broad principles of management which are as follows: (1) Surgical resection of localized M. abscessus lung disease combined with multidrug clarithromycin-based therapy offers the best chance for cure. As such there are so far no proven or predictable efficacious drugs for the treatment of M. abscessus lung disease. (2) Treatment of nonpulmonary disease caused by RGM (M. abscessus, M. chelonae, M. fortuitum) should be based on in vitro susceptibilities. (3) Surgical debridement may be an important component of management in some cases. [39] Medical treatment of RGM infections is difficult as prolonged duration of therapy is required and also some of the antimicrobials are expensive and may have side effects. There is an urgent need to conduct studies in India regarding antimicrobial susceptibility patterns as it could be quite different from the western scenario. There are several papers from various countries in which susceptibility of M. fortuitum to amikacin, imipenem, ciprofloxacin, clarithromycin, sulphonamides, and cefoxitin ranges from 96 to 100%, 61 to 98%, 62 to 100%, 30 to 84%, 6 to 100%, and 19 to 56%, respectively. [49],[58],[59],[60] Susceptibility of M. abscessus from Korea and Taiwan to amikacin, imipenem, ciprofloxacin, clarithromycin, doxycycline, sulphamethoxazole, and cefoxitin has been 94-96%, 8-12%, 3-44%, 79-83%, 0-8%, 1-12%, and 3-11%, respectively. However, the antimicrobial susceptibility of RGM isolated in Texas showed that all M. fortuitum isolates were susceptible to amikacin and ciprofloxacin, 81% to imipenem, 71% to trimethoprim-sulphamethoxazole (TMP SMZ). Of the M. abscessus 98% were susceptible to clarithromycin, 75% were susceptible or intermediately susceptible to cefoxitin and a few (<20%) were susceptible to ciprofloxacin, TMP SMZ and minocycline. [61] A study on antibiotic susceptibility pattern of RGM in India showed all M. abscessus isolates to be resistant to tobramycin and susceptibility to amikacin, gatifloxacin, and moxifloxacin was found to be 98%, 91%, and 88%, respectively. M. fortuitum isolates showed the following sensitivity: Amikacin (100%), gatifloxacin (92%), moxifloxacin (86%), ciprofloxacin (86%), norfloxacin (74%), and azithromycin (64%). Majority of the RGM were resistant to ceftazidime, cefotaxime, and cefoperazone. [62] However, the susceptibility was done by the disc diffusion method. In a study done at our tertiary care centre, we found M. chelonae and M. abscessus to be resistant organisms. We have also found M. fortuitum resistant to clarithromycin. [63] Many studies have shown that M. fortuitum contains an inducible erythromycin methylase gene erm which may confer macrolide resistance. Some investigators believe that differences in antibiotic resistance rates in RGM maybe the result of population or geographical differences or may be due to the method of susceptibility testing. One important distinguishing feature of isolates of the M. smegmatis group in contrast to the M. fortuitum group and the M. chelonae abscessus group is their lack of susceptibility to the new macrolides including clarithromycin. Therefore it becomes important to identify RGM isolates to exclude groups like the M. smegmatis group and the M. fortuitum third biovariant sorbitol positive group which are intrinsically resistant to macrolides. Prevention The recommendations by the ATS/IDSA for prevention of healthcare-associated outbreaks and pseudo outbreaks emphasises avoidance of the following: (1) Contact or contamination with tap water in patients with indwelling central catheters. (2) Usage of tap water for cleaning of endoscopes. (3) Multidose vials for injections. (4) Tap water or ice prepared from tap water in the operating room especially during cardiac surgery or augmentation mammaplasty. [39] Conclusion The RGM have continued to emerge as important human pathogens that can cause a variety of diseases from localized cutaneous infections to disseminated disease. The RGM have been responsible for a number of healthcare-associated outbreaks and pseudo-outbreaks. Types of clinical disease and the antimicrobial susceptibility often differ for individual species of RGM. The most common taxonomic error is the failure to separate the two distinct species of M. chelonae and M. abscessus in the laboratory. The two species not only differ in clinical disease, but also in susceptibility to drugs. Hence, it is important to identify the two species in the laboratory. The statement published by ATS/IDSA suggests the following for RGM: RGM isolates should be identified to the species level using a recognized acceptable methodology, such as PCR REA or biochemical testing, not HPLC alone; routine susceptibility testing for both taxonomic identification and treatment of RGM should be done with amikacin, cefoxitin, clarithromycin, ciprofloxacin, doxycycline, linezolid, TMP SMZ, fluorinated quinolones, tobramycin (for M. chelonae only), and imipenem (for M. fortuitum only); communication between clinician and laboratorian is very important in order to determine the importance and extent of identification for a clinical RGM isolate. To conclude it is extremely important to differentiate RGM to the species level and perform susceptibility testing in order to choose the most effective drug therapy. This will also go a long way in monitoring the development of drug resistance which may occur with prolonged therapy. Thus there is a need to create awareness among clinicians and microbiologists so that necessary steps can be taken to diagnose and appropriately treat infections with RGM. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11086t3.jpg] [mb11086t1.jpg] [mb11086t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}