 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 353-358 Review Article Transfusion-transmitted hepatitis E: Is screening warranted? M Bajpai1, E Gupta2 1 Department of Transfusion Medicine, Institute of Liver and Biliary Sciences, Sector D1, Vasant Kunj, New Delhi 110 070, India Date of Submission: 02-May-2011 Code Number: mb11087 PMID: 22120793 Abstract Hepatitis E virus (HEV) is an emerging infectious threat to blood safety. In recent years, there have been a number of publications delineating this threat by providing evidence of the transmissibility of this virus through transfusions. The extent of transmission and its clinical relevance are issues under debate at present. HEV usually causes a self-limiting illness which subsides in a few weeks barring a few cases where fulminant hepatic failure occurs. The virus poses a risk of higher morbidity and mortality in pregnant females, patients with pre-existing liver disease and solid organ transplant recipients. As these categories of patient often require repeated transfusions or massive transfusions, they are exposed to a greater risk of transmission of HEV. At present, there is little evidence to advocate universal screening for this virus but considering that there is no definitive treatment for HEV induced hepatitis, selective screening should be advocated in blood products for high risk recipients in endemic areas.Keywords: Hepatitis E virus, transfusion transmitted viruses, blood products Introduction Transfusion safety has always been a major concern for blood transfusion services and efforts to make blood transfusions safer are constantly being made through measures such as stringent donor screening, special precautions during phlebotomy such as diversion pouches, screening blood for markers of transfusion transmissible infections, pathogen inactivation of blood and shortening the shelf life of platelets. In spite of all these developments, blood is not and may never be 100% safe. This is because new and emerging viruses as well re-emerging old viruses may pose a yet undefined risk to transfusion safety. The extent of this risk is not always clearly delineated. Hepatitis E virus (HEV) is one such virus about which a significant number of studies have been published in the last decade regarding the risk it poses to transfusion safety. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10] This virus was first recognized retrospectively from samples collected during an epidemic in Delhi in 1955. [11] Later, it was identified to be Hepatitis E during an epidemic in Kashmir in 1978. It is a cause of wide-spread water-borne epidemics and sporadic infections in developing countries. This virus usually causes an acute self-limiting hepatitis, but in some cases fulminant hepatic failure (FHF) with resultant mortality and morbidity may occur. Pregnant females and patients with pre-existing liver disease are at an increased risk of FHF. These categories of patients often require repeated transfusions or massive transfusions and as a result they are exposed to a greater risk of transfusion transmitted infections. Taking into consideration the above observations, HEV needs to be evaluated in the context of the risk it poses to transfusion safety. The important aspects of HEV with respect to risks regarding blood transfusion safety need to be clarified. The issues that will be discussed are
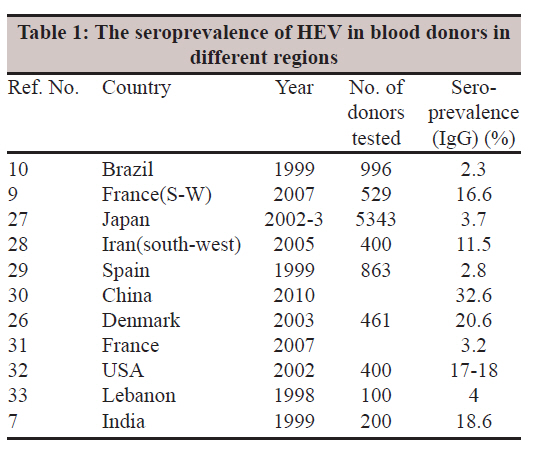
The present review will attempt to provide a comprehensive view of the various aspects of decreasing the risk posed by this virus to blood safety and a discussion on future perspectives on the issue of screening for this virus. Hepatitis E virus HEV is the sole member of the genus Hepevirus in the family of Hepeviridae. [12] It is a round non-enveloped virus 27-34 nm in diameter with a genome of 7.2 kb that consists of a single-stranded RNA containing three discontinuous and partially overlapping open reading frames (ORFs). There are four major genotypes of HEV (1, 2, 3 and 4) and a single serotype. Genotypes 1 and 2 are considered human viruses, while genotypes 3 and 4 are zoonotic and have been isolated from humans and animals. [13] HEV transmission has been shown from pigs to humans. In addition, other animals such as boars, deer, cows, sheep, goat, horses and rabbits have been shown to be susceptible to infection and acting as reservoirs for HEV in nature. [12] Genotype 1 is prevalent in Asia and Africa and genotype 2 in Mexico and Africa, while genotype 3 has a worldwide distribution. Genotype 4 is mainly restricted to India and East-Asian countries. [13] HEV genotype 1 is more conserved and is classified into five subtypes: 1a, 1b, 1c, 1d, and 1e. Genotype 2 sequences are classified into two subtypes: 2a and 2b. Genotypes 3 and 4 are extremely diverse and are divided into 10 and 7 subtypes respectively. [14] These genotypes and subtypes are helpful in understanding epidemiological characteristics of the virus such as geographical spread or transmission in the community. Epidemiological characteristics The epidemiological pattern of HEV infection in humans include periodic outbreaks or sporadic cases in endemic areas, sporadic cases seen in travellers in areas of low endemicity and more recently autochthonous (locally acquired) hepatitis E in developed countries that suggests zoonotic transmission. [15] Transmission of HEV occurs predominantly by the faecal oral route although parenteral and perinatal routes have been implicated. [16] The outbreaks are usually waterborne and are more common during periods when faecal contamination of the water supply is likely. This usually occurs after monsoon due to floods as well as during periods of water scarcity when faecal matter in water bodies becomes concentrated. Cases are often reported after eating food (usually infected meat) from a common source. [16] During epidemics, attack rates of 1-15% are seen with a case fatality rate of 0.2% to 4%. The attack rates are higher for males as compared to females and young adults as compared to children. [17] Children present with the anicteric form of the disease more often than adults (21.8% vs. 14.6%). [18] A significantly higher rate of 10-20% of fulminant hepatic failure has been observed in pregnant women especially during the third trimester. [19] The attack rate has also been reported to be higher in pregnant females as compared to non-pregnant females of child bearing age. The prognosis is also poor in patients with pre-existing liver disease. [13] Person to person transmission is unusually low, with second attack rates in household contacts being as low as 0.7-2.2%. [17] Recently, significant person to person transmission has been reported in Uganda. [20] Epidemics of hepatitis E usually occur in unimodal outbreaks with a highly compressed curve of incidence or, alternatively, prolonged epidemics with multiple peaks of incidence. HEV is a major cause of sporadic hepatitis and more than 25% of acute sporadic hepatitis is attributed to hepatitis E in endemic areas. In India, up to 30-70% of acute sporadic hepatitis is attributed to HEV. [21] Sporadic cases may be attributed to faecal contamination of food and water. [17] A study from North India found HEV genomic sequences in 40% of the sewage specimen in a city. [22] In another recent study from Gokulpura area of Delhi, HEV RNA was detected in 4.25% of sewage samples and 1.42% of drinking water samples. An interesting correlation was that 29.8% cases of viral hepatitis in the community were due to HEV. [23] Egypt presents an entirely different sero-epidemiological pattern which is similar to that of HAV. There is wide spread exposure to the virus at an early age with a seroprevalence of 60% or more in the first decade. [24] This results in sporadic cases of HEV hepatitis but no periodic out breaks as in India. In developed countries, a number of cases have been due to zoonotic transmission but it cannot explain all the cases. These may be due to a continuous circulating pool of persons with subclinical HEV infection. Most persons who have anti-HEV antibodies do not recall having an episode of jaundice; this suggests that a large proportion of HEV infections are subclinical in nature. [13] This is of great importance when we consider transfusion transmissibility of HEV because donors may have never had jaundice at all. Seroprevalence The presence of anti-HEV IgG antibody has generally been taken as evidence of prior exposure to HEV. The duration of persistence of circulating IgG anti-HEV antibodies remains unclear. IgG antibodies to HEV are detected very strongly during the acute illness and may persist for up to 12 years or more. [25] There are characteristic regional variations in the age, gender and urban/rural seroprevalence of HEV. The seroprevalence in blood donors in different regions is shown in [Table - 1]. [1],[7],[9],[10],[26],[27],[28],[29],[30],[31],[32],[33] In western countries, the seroprevalence of HEV IgG antibodies varies from 1% to 20%. [17] In most developed countries, the prevalence is in the range of 2-4% in blood donors. Recently, blood donors in south west England and South west France have shown higher prevalences of 16% and 16.6% respectively. [9],[15] A study from Denmark which was done on samples from donors in 2003 and archived donor samples from 1983 showed a decrease in the seroprevalence from 32.9% to 20.6% during this period which is unexpectedly high. [34] A similarly high seropositivity was seen in USA where 18-21% of blood donors had antibodies to HEV. [13] Recently, questions have been raised regarding the accuracy of the research assays used in both the above studies which are from the same source. [20] Endemic regions have a very high seroprevalence. In India, the seroprevalence of HEV IgG in young adults is around 20-40%. [33] In India, seroprevalence of HEV rises with age peaking in young adults but studies from China, Japan and Denmark have shown a continuous rise in prevalence with age with peaks at around 60 years or higher. [13] In contrast, in Egypt, 65% of the children below 10 years are HEV seropositive suggesting a widespread exposure early in life. [19] In many regions, there is a male preponderance in HEV seropositivity (Japan, Iran), while in other regions there is no gender variation in seroprevalence (France, Brazil). [10],[11],[35],[36] The reasons for variation in patterns of seroprevalence with respect to region, gender and age are still not clear and need further studies. The natural history of the disease caused by the virus, chronicity, long-term sequelae and treatability HEV hepatitis has varied manifestations extending from an acute self limiting illness to fulminant hepatic failure. [17] There is increasing evidence from endemic regions that asymptomatic infections comprise a major chunk of the disease burden. [13] Although HEV hepatitis has been classically described as an acute illness, recently there have been reports of chronicity in immunosuppressed patients. [37] The hepatitis caused by HEV usually presents as a self-limiting illness and the symptoms include malaise, fever and gastrointestinal symptoms. Jaundice follows after the prodromal symptoms subside although at times there may be anicteric hepatitis. Laboratory investigations show an increased conjugated bilirubin and alanine aminotransferase; deranged coagulation parameters may also be seen. [13] The illness usually resolves within a month. A small subset of patients may develop prolonged illness with cholestasis. [18] Fulminant hepatic failure due to massive liver necrosis is seen in a small subset of patients who present with encephalopathy and coagulation disorders. Mortality is high in these cases. [13] Pregnant women especially those in the third trimester are at a disproportionately higher risk of developing fulminant hepatic failure with adverse outcome for both mother and the foetus. [13] Mortality rate of up to 20% is seen in this subset of patients. A study from India on 97 pregnant women with acute viral hepatitis has shown HEV to be causative in 36.2% of the cases contributing to 75% of the cases with FHF and responsible for 75% of mortality. [38] Another patient group which has higher morbidity and mortality associated with HEV infection are patients with pre-existing liver disease. HEV is responsible for rapid decompensation and death in patients with chronic liver disease of diverse aetiology such as chronic hepatitis B and C, Wilson′s disease and autoimmune and cryptogenic liver disease. [13] Chronic HEV infection leading to cirrhosis and liver failure has been described in a liver transplant recipient. The patient had a retransplantation after which chronic hepatitis recurred. [39] In another patient with a similar history but a lower viral load, chronic hepatitis did not recur after retransplantation. Hepatitis E-related cirrhosis has also been seen in other solid organ transplant recipients. [40],[41] Immunocompromised patients on chemotherapy have also shown mild hepatitis with prolonged viral shedding. Curiously patients with HIV who are also immunocompromized have not shown such chronicity. [13] The natural history of HEV infection differs between developed and developing countries. Periodic outbreaks have been reported in developing countries while almost an equivalent seroprevalence among the population no outbreaks have been reported from developed countries suggesting predominantly subclinical infection. [20] This is one of the many riddles HEV poses on us. Is HEV transfusion transmissible? In order to be transmissible through blood there should be a period of asymptomatic viraemia or the infection should be subclinical in a proportion of the infected population. Viraemia in individuals infected with HEV is usually of a short duration with a brief incubation period followed by symptomatic phase. The viraemia disappears before complete resolution of symptoms and there is no chronic carrier state. There are reported instances where the viraemia may be protracted as after acute HEV hepatitis in children. [42] Prolonged viraemia extending beyond 3 years has also been seen in renal transplant patients or in those on immunosuppressive therapy although they do not pose a threat to the blood safety as they would not be eligible as donors. [19] In recent years, studies have shown asymptomatic viraemia in blood donors which is suggestive of ongoing subclinical infection. In a study by Gotanda et al. of 6700 Japanese blood donors with elevated ALT, 479(7.1%) were HEV seropositive of which 6 had detectable HEV RNA In blood. Three donors, seronegative for HEV, also had detectable HEV RNA. [4] In another study, Sakata et al. have shown the presence of HEV RNA in blood donors with elevated ALT levels. [2] Arankalle and Choube from Pune, India, have shown 1.5% (3/200) of blood donors to be positive for HEV RNA and suggested the possibility of transmission by transfusion. [6] The above studies show that HEV RNA is present in the serum of healthy blood donors and there is a potential risk for transmission of HEV through blood. Boxall et al. from UK have shown transmission of HEV from a donor to recipient which was proven by serology and molecular methods. The infection in the recipient was asymptomatic apart from mild jaundice and elevated ALT. The donor developed symptoms on day 14 after receiving a blood donation and had asymptomatic viraemia during this period. [43] Similar cases have been reported by Colson et al. and Matsubayshi et al. [3],[8] Clinical relevance of transfusion-transmitted HEV Retrospective studies in transfusion recipients have been inconsistent. Studies from non-endemic areas have shown no clear association of HEV seroprevalence with previous transfusion, while studies from endemic areas have suggested the possibility of transmission through blood transfusion on retrospective evaluation in transfusion recipients. [44],[45],[46],[47],[48] Khuroo et al. in a study from Kashmir, India, have shown a significantly higher prevalence of markers for acute HEV (anti-IgM and HEV RNA) in multitransfused patients (13/145) as compared to controls (2/250). They have also shown that patients positive for HEV markers had received more transfusions, had a higher incidence of icteric disease and higher ALT levels. [5] Arankalle and Choube from Pune and Irshad and Peter from Delhi have also shown a significantly higher prevalence of markers of acute HEV in transfusion recipients. [6],[48] In endemic areas, therefore, there is a definite risk of transfusion transmitted HEV. In cases where proven transmission has occurred, the infection has been asymptomatic or presented as a mild self-limiting illness. [49] The effects of transmission of HEV through blood have not been described in the subset of patients at high risk of fulminant hepatic failure such as pregnant females, patients with pre-existing liver disease and solid organ transplant recipients. These patients may not have an uneventful recovery and may need more comprehensive preventive measures against HEV. Is transfusion transmitted HEV preventable through donor screening? Are there quick, reliable and affordable tests available to screen the virus in blood? HEV can be easily diagnosed through simple laboratory serological tests. In general, approximately 95% of acute HEV infections are detected as being reactive for IgM class antibodies. Hence, if donated blood is carefully screened by any of the commercially available kits from reputed and reliable firms (see below) for the presence of IgM antibodies to HEV, transmission maybe prevented. IgM antibodies to HEV are present during the acute phase of infection and disappear within several weeks after symptoms have resolved. Serological-based assays especially IgM antibody detection have good sensitivity and specificity. IgG class antibodies too are detected very strongly during the acute phase of infection and are known to persist for several months. [24] Many commercial ELISA-based tests are present based on indirect antibody detection. At present, it is generally agreed that HEV antibody tests based on ORF2 of HEV have broad activity and yield data that are reproducible in many laboratories and definitely are superior to tests based on combinations of ORF2 and ORF3 antigens of HEV. [50] Two HEV antibody assays available commercially, i.e. Abbott Immunoglobulin G Assay (Abbott Laboratories, Wiesbaden, Germany) and Genelabs IgG Assay (Genelabs Diagnostics, Singapore, Singapore) have been evaluated and were found to have adequate sensitivity and specificity. [51] Molecular tests based on HEV RNA detection are not warranted for screening or even diagnosis of HEV infection. They are usually used for epidemiological studies and genotyping of the virus. It has many limitations such as being less sensitive, labour intensive, cumbersome and expensive. Moreover HEV viraemia is short lived approximately 20 days and is always coincidental with acute phase of illness. Studies have shown viraemia in about 0.1-2% in HEV IgM positive selective blood donors. [2],[4] Hence, by careful screening by reliable simple serological tests, HEV infection clinically or sub-clinically can be detected. At present, IgM ELISA would cost around 100-150 per assay and can be carried out within 2-3 h in a routine Blood bank setting. Conclusions In the light of present knowledge, as there is no clear cut association of transfusion with HEV infection as exists for HBV and HCV, but nevertheless transmission of HEV does occur and may be more common in endemic areas. There is no evidence of significant morbidity in most recipients and as of now we do not feel that screening of all blood for HEV is warranted. However, knowledge regarding the serious consequences of HEV in certain subsets of patients and taking into consideration that there are no definitive treatment modalities for HEV hepatitis and no licensed vaccine available at present, serious consideration should be given to selective screening for patients at high risk for fulminant hepatic failure or chronicity. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11087t1.jpg] |
| |||||||||
{kind=link}