 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
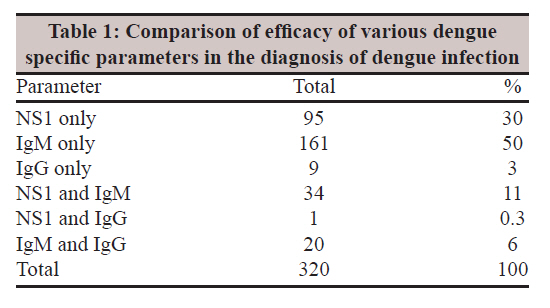
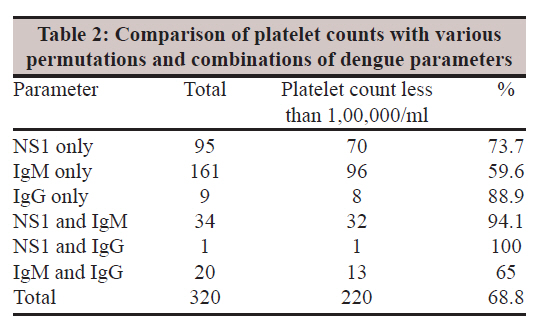
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 359-362 Original Article Association of platelet count and serological markers of dengue infection- importance of NS1 antigen RD Kulkarni, SS Patil, GS Ajantha, AK Upadhya, AS Kalabhavi, RM Shubhada, PC Shetty, PA Jain Department of Microbiology, SDM College of Medical Sciences and Hospital, Sattur, Dharwad 580 009, Karnataka, India Date of Submission: 23-Jun-2011 Code Number: mb11088 PMID: 22120794 Abstract Introduction: Dengue is an acute viral infection with potential fatal complications. Specific antibody detection has been the mainstay of diagnosis which is prone for both false positive and false negative reactions. The newer parameter NS1 appears to be highly specific and reliable for diagnosis of dengue infection from the first day of fever. Platelet count is the only accessory test for diagnosis of dengue infection in the peripheral laboratories. Therefore, we tried to evaluate the association of platelet counts against NS1 and IgM/IgG in dengue infections. Keywords: Dengue, IgM, IgG, NS1, thrombocytopenia Introduction Dengue is an acute, potentially fatal viral infection that can culminate into dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS). It is caused by four serotypes of dengue virus (DV), namely DEN-1, DEN-2, DEN-3 and DEN-4 belonging to genus Flavivirus and family Flaviviridae. It is spread through the bite of infected Aedes aegypti mosquito. [1] Most primary infections are uneventful. Infection with one serotype confers an individual life-long immunity to that serotype and cross-reactivity to the other serotypes. The complications like DHF and DSS are usually attributed to this cross-reactivity. [1],[2] Dengue is almost endemic throughout India. The resource poor health care system has to depend upon simple to perform and easy to interpret laboratory tests for diagnosis. It is known that early and specific diagnosis of DHF or DSS followed by supportive therapy reduces morbidity and mortality. [3] The variability in the clinical illness associated with dengue infection (DI) cannot be accommodated in a single clinical definition. However, confirmation of DI is the most essential pre-requisite in the management of complications. [4] The ′gold standard′ tests for identification of DI are not within the reach of peripheral and even most tertiary care laboratories. Detection of dengue specific IgM/IgG has been the mainstay of diagnosis of DI. Antibody detection is an indirect method of diagnosis and, therefore, is prone to false positive as well as false negative results. [5] Of late, non-structural protein 1 (NS1) detection is available for diagnosis of DI. [6] NS1 detection is reported to be sensitive as well as highly specific. [7] Apart from the dengue specific parameters, platelet count is the only accessory laboratory test available in the peripheral areas that can support the diagnosis of DHF or DSS. Even in remote areas, platelet counts can be roughly estimated by microscopy. [8] Keeping in mind the logistic constraints of healthcare system in the peripheral areas, we tried to correlate the platelet counts and immunochromatography (ICT)-based dengue serology tests. Materials and Methods The study was conducted at a tertiary care teaching hospital from July 2010 to January 2011 after receiving permission from the institutional ethical committee. A total of 2104 serum samples from equal number of clinically suspected dengue fever were collected. Since our laboratory works round the clock, the samples were tested immediately for NS1, IgM and IgG by ICT-based tests. The test kits used were Advantage dengue NS1 Ag and Ab Combi Card supplied by J Mitra and Co. Pvt. Ltd, New Delhi, India. The tests were performed strictly as per the manufacturer′s instructions. Platelet counts of all the cases positive for any of the dengue parameter were recorded. Platelet counts were also recorded in 150 cases of fever that were negative for any of the dengue parameter. The permutations and combinations of dengue-specific parameters were correlated with thrombocytopenia using standard error of proportions test. This evaluation has been done keeping in view the scenario at the peripheral centres, where only ICT-based tests are available for diagnosis of DI. No healthy controls were included in the study as it has been amply proved that NS1 positivity is negligible in this group. Results Of the 2104 serum samples tested, a total of 320 specimens were tested positive for either one or more of the three markers (NS1, IgM and IgG) tested. Of the 320 serum samples, 95 (29.68%) patients were positive for NS1 only, 161 (50.3%) positive for IgM only, while 9 patients had only IgG. More than one marker was detected in the remaining 55 (17.18%) samples [Table - 1]. Platelet count less than 1, 00,000/ml was noticed in 220 cases (68.75%). Of the 150 cases presenting with fever that were negative for any of the dengue-specific parameters by ICT, 45 showed thrombocytopenia (30%) [Table - 2]. Discussion For a long time detection of dengue-specific IgG/IgM has been the mainstay of diagnosis of DI. The dengue-specific antibodies begin to appear only around fifth day of fever in primary infection. [5] Even in most secondary infections, both the IgM and IgG type antibodies cannot be recorded before third day. [9] Therefore, there is always a window period, both in primary and secondary DI when only antibodies are tested. The new parameter, now available, for diagnosis of DI, the NS1 antigen, is detectable from day 1 of fever both in primary and secondary infections. It is important to note that NS1 is shown to be highly specific viral marker making it extremely reliable parameter for the diagnosis of DI from day 1 of the fever. [10] The distribution of various dengue specific parameters is shown in [Table - 1]. Of the 320 cases, 95 (30%) were positive for only NS1 antigen. Considering very high specificity of NS1 it can be stated that we would have missed the diagnosis in 30% cases had we not included NS1 in the test panel. [11],[12] Datta (2010) and Shrivastava (2011) have shown that NS1 was positive in 140 out of 600 (23.3%) and 15 out of 91 (16%) cases respectively in their studies. [10],[13] This supports the fact that a large number of cases would be missed if NS1 is not included in the test panel. NS1 alone or in combination with either IgM or IgG was positive in 130 cases (40.6% cases) in our study. Among two antibodies, IgG is a less reliable marker in the diagnosis of DI. [5] Both clinical and sub-clinical infections can produce IgG which may persist for several years affecting the interpretation of test results. [14] It is highly likely that IgG levels could be higher in endemic areas because of bites from infected mosquitoes. However, dengue-specific IgM is a very good indicator of recent infection. It may also be detectable in secondary DI. [5] Utility of antibody in the diagnosis of infections relies mainly on rising titres, especially in the endemic areas. However, repeat testing of cases, for the same infection, when the first test is negative or sending samples for determination of rise in titre is ′almost never′ utilized in clinical practice. When NS1 is positive, there is no need of repeat testing as it is a highly specific marker of DI. [5] We tried to find the association of dengue parameter positivity with thrombocytopenia. The comparison of platelet counts with different dengue specific parameters is shown in [Table - 2]. Of the 320 cases, 220 (68.8%) showed thrombocytopenia. In 130 cases that were positive for NS1, thrombocytopenia was evident in 103 (79.2%) cases. In contrast, when only antibodies were considered for the diagnosis of DI, thrombocytopenia was noted in 117 of 190 (61.6%) cases only. Association of thrombocytopenia with NS1 was found to be higher by SEP test = 5.01, Z=3.51 and P value <0.001, highly significant. Further analysis of two groups NS1 only (73.68%) v/s NS1 plus IgM (94.12%) showed that thrombocytopenia was associated excellently when both NS1 and IgM were positive compared to NS1 alone (SEP = 6.06, Z=3.37, P<0.001, highly significant). The role of antibody in the pathogenesis of dengue fever is well-known. Therefore, better association of platelet count with detection of antibody is consistent. Platelet counts are decreased in several other conditions like some viral infections other than dengue, drug induced thrombocytopenia, collagen vascular diseases, idiopathic thrombocytopenia etc. [3] We therefore, tried to correlate platelet counts in cases of fever that tested negative for any of the dengue parameters. In 150 cases of fever, in which none of the dengue parameters was positive, thrombocytopenia was noted in 30% cases (45 of 150). Applying SEP test for association (SEP = 4.55, Z=8.51, P<0.001) it was found that association of thrombocytopenia and dengue parameter was significantly higher compared to thrombocytopenia in dengue negative cases. This study has been carried out at a tertiary care teaching hospital. It is worth mentioning here that most tertiary care teaching hospitals lack in viral culture setup. Therefore, applying gold standard tests in studies related to viral infections is out of reach of these centres. Dengue is an infection that is present in urban, semi-urban and rural areas. Our healthcare system is extremely resource poor. Top class technological backup is available only at very few elite laboratories situated in big cities. It is important to conduct studies in the peripheral centres where the laboratory has to function without great technological backup and still is expected to provide reasonable opinion to the clinician in the management of infections like dengue. The limitation of the present study was that enzyme linked immunosorbent assay (ELISA) for qualitative or quantitative detection or Polymerase Chain Reaction (PCR) could not be used. ELISA has higher sensitivity than ICT-based tests. [12] Inclusion of ELISA in this study could have given us an opportunity to comment on the efficacy of ICT to identify DI. Most of the cases coming to our hospital were referred from various places and had received a few days treatment before reaching this hospital. The precise day of fever at the time of conducting the test could not be obtained in a large number of cases. In spite of this, NS1 only was positive in 30% cases. Given an opportunity to test every case of fever on day 1, more number of cases could have been picked up by NS1. It is shown that the titres of NS1 represent the viral load and the viral load is directly proportional to complications. [7] It can be logically inferred that in complication prone cases, i.e. having higher viral load, detection of NS1 will be easier because of higher NS1 levels. This would reduce the chances of false negativity by a less sensitive test like ICT. We therefore feel that inclusion of NS1 in the test panel either in micro-ELISA or ICT test format must be included for evaluation of all cases of fever, either in endemic or non-endemic areas. The ease, speed and dependability of ICT make it an excellent tool in addressing this potentially fatal, epidemic prone infection that has become an important public health problem in our country. One can never forget the fact that dengue often breaks out in resource poor peripheral areas where ICT-based tests could be the only support available. Acknowledgement We thank sincerely to Dr. K. R. Pravinchandra, Associate professor, Dept. of Community Medicine, SDM College of Medical Sciences and Hospital, Dharwad for the statistical analysis of the data. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11088t2.jpg] [mb11088t1.jpg] |
| |||||||||

{kind=link}
{kind=link}