 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
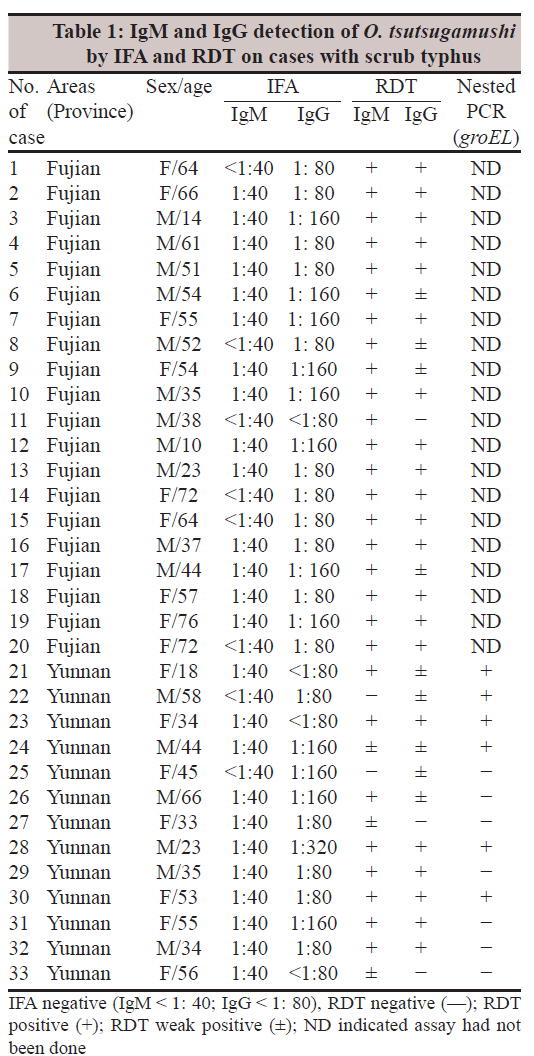
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 368-371 Original Article A rapid, sensitive and reliable diagnostic test for scrub typhus in China Zhang Lijuan1, He Si2, Jin Yuming3, Li Liang3, Li xuemei4, Liu Lianying5, Yu Huilan1, Yu Qiang6, Chen Chuangfu7, Wang Shiwen1 1 Department of Rickettsiology, National Institute of Communicable Disease Control and Prevention, China CDC, Changping P.O. Box 5, Beijing 102206, China Date of Submission: 10-Jun-2011 Code Number: mb11090 PMID: 22120796 Abstract Purpose: To evaluate the performances for detection of IgM and IgG antibodies to Orientia. tsutsugamushi (Ot) using a gold conjugate-based rapid diagnostic test (RDT). Keywords: Colloidal gold, Orientia tsutsugamushi, rapid diagnostic test, rapid diagnosis, scrub typhus Introduction Scrub typhus is a acute febrile rickettsial diseases caused by the pathogenic agents of Orientia tsutsugamushi (Ot) and is widely distributed in China. [1],[2] Outbreaks of scrub typhus have been frequently reported in recent years. [3],[4] Nearly all cases are diagnosed based on the clinical features and experimentally treated without laboratory confirmation. The golden micro-indirect fluorescence assay (mIFA) proposed by the WHO collaborator center of rickettsiae have not been popularized because of limited instruments of fluorescence microscopy. Delay in diagnosis and treatment of scrub typhus often causes multi-organ failure and an increasing in mortality. It is reported that the mortality of untreated scrub typhus is up to 35%. [5] A reliable and rapid diagnostic reagent is urgently needed to be developed for national wide application in China. Here, we evaluated a novel RDT for detecting specific IgM and IgG antibodies to O. tsutsugamushi from patients suffering from scrub typhus. Materials and Methods Description and confirmation of cases Thirty three patients were all from endemic regions of scrub typhus in China, including 20 from suburbs of Fuzhou City in 2009, the capital of Fujian province and 13 from Yuxi City, Yunnan province, in 2005. [6] The average age of patients was 47 year old (range from 10 to 76 years old). All cases were characterized by high fever (ranged from 38°C to 41.5°C), headaches, and weakness. Eschars were noticed on bodies and extremities of 13 patients from Yunan province [Figure - 1] but no rash was observed. Twenty cases from the Fujian province were recovered by oral administration doxycycline, while 13 patients from Yunnan province were treated by oral chloramphenicol. Diagnosis of scrub typhus was confirmed by typical clinical presentation and laboratory assays including detection of IgM and IgG antibodies against O. tsutsugamushi and nested PCR targeting groEL gene of O. tsutsugamushi. [7] This study was approved by the Human Research Ethics Committee of Chinese Centre for disease control and prevention (China CDC). Sera Thirteen sera samples from Yunnan province and 20 sera from Fujian province were collected at acute stage of illness (2 to 10 days after onset of illness) in 2005 and 2009 respectively and they were kept at -80°C until the present study. In addition to these 33 sera, 94 positive sera samples were collected from farmers from endemic areas of the Jiangsu province and the Hainan province respectively and IgG antibodies against O. tsutsugamushi were tested by IFA and they were confirmed by a positive reaction. Eighty-two sera from blood donors were collected from healthy farmers in Guangde County (50 sera) and Mingguang County (22) of the Anhui province respectively, and 10 from Tongzhou districts of Beijing City in 2009. The 15 reference rabbit sera immunized with 12 members of order Rickettsiae (C. burnetii, R. typhi, R. heilongjiangensis, R. sibirica, R. austrilia, R. prowazekii, R. conorii, R. parkeri, B. henselae, B. quintana, E. chaffensis, A. phagocytophilum, and with another 3 non-rickettsia agents, E. coli 157, Lp1 and B. melitensis) were also included in the negative control panel, which were tested to observe if cross-reaction occurred. In addition, four reference sera consisting of Ot serotypes Karp, Kato, TH187, and TA 736 were detected by the RDT. mIFA mIFA were performed as previously described. [8] Briefly, sera were serially diluted 1:10, 1:20, 1:40…. in PBS with 3% skimmed milk powder and 25 ml of the diluted serum was placed in appropriate wells of the antigen slides (prepared by culture O. tsutsugamushi serotype Karp in Vero cells in our Lab) and incubated for 60 min in a moist chamber at 37°C. After washing to remove unbound antibody, slides were reacted with FITC-conjugated goat anti-human immunoglobulin (IgM or IgG, Sigma Co.) as a secondary antibody. The stained slides again rinsed and counterstained with Evan′s blue before examination using a fluorescent microscope (Nikon-E400-FL-F-A, Nikon Corporation, Japan). Samples were interpreted as reactive when clear fluorescent bacterial morphology was evident. Samples reactive as the 1:80 screening dilution were deemed positive. To detect IgM antibodies, the procedure was the same as IgG antibody test except RF-absorbent (Behring Diagnostics, Marburg, Germany Behring) was used to absorb the IgG antibodies before diluting sera. Dilutions with 1:40 or larger reaction with antigen were considered positive. Rapid diagnostic test RDTs employed a mixture of recombinant 56-kDa proteins from different Ot serotypes including the Karp, Kato, TA736, and TH187 strains of O. tsutsugamushi as antigen. [9],[10] The RDTs were manufactured and donated by InBios International, Inc. Seattle, USA, for this study. The test procedure was briefly as following: 3 drops (120 ml) of IgM or IgG chase buffer is added to a plastic well and add 5 ml of sera to the sample pad area of the test strip, followed by placing each test strip with samples applied into individual wells containing chase buffer and read the results in 15 min. The control line (C) and test line (T) appear (purple-red band) concurrently as regarding as positive. The test is considered as negative when only the control line appears. The test is invalid if no control line appears. Limit of detection Twenty-five IgM positive sera and 29 IgG positive sera listed in [Table - 1] were randomly selected to be further serially diluted as 1:10, 1:20, 1:40 ……., and then detected by the RDT so as to determine the lowest detection limit. Statistical analysis Statistical analysis was conducted using SAS software (version 9.1). Comparison of the positive rates between RDT and mIFA assays was performed by using the χ2 test and the P value level was used to determine the significance and the P value of ≤0.05 was considered significant. Results Control sera Eighty-two control sera from healthy farmer were confirmed to be negative by IFA (titres of IgM were <1:40 and titres of IgG were <1:80). All these sera were then tested by the RDT and results showed no positive reaction. For the detection of 94 positive sera (GMT by IFA:160 (80-640) from the Jiangsu and Hainan provinces respectively, the coincidence rate between the RDT and IFA was 100%. Here we concluded that the RDT was dominantly sensitive than IFA for early diagnosis of scrub typhus. Reference sera Reference sera immunized with 12 individual members of order Rickettsiae including C. burnetii (titre of IgM and IgG by IFA: 1:160; 1:128), R. typhi (titre of IgM and IgG by IFA: 1:80; 1:512), R. heilongjiangensis (titre of IgM and IgG by IFA: 1: 1:80; 1:512), R. sibirica (titre of IgM and IgG by IFA: 1:1:80; 1:512), R. australis (titre of IgM and IgG by IFA: 1: 1:80;1:128), R. prowazekii (titre of IgM and IgG by IFA: 1: 1:80; 1:512), R. conorii (titre of IgM and IgG by IFA: 1: 1:80; 1:512), R. parkeri (titre of IgM and IgG by IFA: 1: 1:80; 1:512), B. henselae (titre of IgM and IgG by IFA:1: 1:80;1:512), B. quintana (titre of IgM and IgG by IFA: 1: 1:80; 1:512), E. chaffensis (titre of IgM and IgG by IFA: 1: 1:80; 1:512), A. phagocytophilum (titre of IgM and IgG by IFA: 1: 1:20; 1:64) and 3 non-rickettsia pathogen including E. coli 157 (titre of IgM and IgG by IFA: 1: 1:40; 1:128), Lp1 (titre of IgM and IgG by IFA: 1: 1:80; 1:512) and B. melitensis (titre of IgM and IgG by IFA: 1: 1:80;1:128) were detected as negative control and results showed no reaction was noticed. Of the 15 reference sera, no cross reaction was observed. However, the 4 reference sera immunized with O.t serotypes Karp, Kato, TH187 and TA 736 were positive. Sera from patients IgM and IgG antibody detection were performed on 33 sera from the acute phase of illness for scrub typhus cases and 94 sera from convalescent stage of the illness by IFA and RDT. For the 33 sera from confirmed cases, the sensitivities of testing IgM by IFA and RDT were 75.6% and 93.9% respectively (P<0.05). For IgG, the sensitivities of IFA and RDT were 87.9% and 90.9% respectively. When IgM and IgG were used together, the sensitivity of IFA and RDT were 96.9% and 100% respectively. LOD The results showed that the sensitivity of the RDT was significantly higher than that of IFA. The GMT of IFA and RDT were 1:37 versus 1:113 respectively (P<0.001) for the IgM test and 1:99 versus 1:279 respectively (P<0.016) for IgG. Discussion In this study, we evaluated the performance of the RDT on 33 sera from the acute phase of illness for scrub typhus cases and 94 sera from the convalescent stage of the illness, and 82 control sera from a healthy farmer donor. The evaluation results showed that the specificity of RDT is as high as 100%, based on the 82 normal human sera and 94 positive sera. Besides the mentioned 82 normal human sera, no false positives were observed on another 12 reference sera immunized with 12 individual members of order rickettsia and 3 sera immunized with 3 individual non-rickettsia pathogens. For Ot serotype TA 736 and TH187, only weak cross reactive was observed. The results of the lowest detection limit for IgM and IgG tests showed that the RDT was more sensitive than the traditional IFA assay. Considering the combined results of IgM and IgG, the sensitivity of the RDT was excellent, 100% sensitive for testing sera from acute-phage of illness (2-10 days after the onset of illness). The average titre of IgM and IgG determined by the RDT was three times higher than that of IFA (P<0.001 for IgM and 0.016 for IgG). The higher sensitivity of RDT is suitable for the earlier diagnoses of scrub typhus during the acute phase of illness, which can avoid delayed treatment and death due to multi-organ failure. Scrub typhus is a national-wide endemic infectious disease in rural areas of China and its diagnosis is also the biggest challenge in China. The significant advantage of the RDT is that it is consisted of several recombinant 56 kD proteins including Ot serotype Karp, Kato, TA736, and TH187, which enhance its sensitivity. Until now, there are a total of eight serotypes of Ot in the world. The major serotypes of O. tsutsugamushi in China are stain Karp, Kato, and Gilliam. A novel serotype of strain Kawasaki has been discovered in recent years. [11] Misdiagnoses and delay treatment of scrub typhus are frequent in rural areas of China, which generally cause multi-organ failure of patients and even death. [12],[13] The traditional gold standard IFA assay could not been used in rural areas because of limited medical sources. [14] A rapid and reliable diagnosis method is urgently needed in China and we believe that the RDT is particularly meeting this purpose. Acknowledgement This project was supported by the National Basic Research Program of China (973 Program) 2010CB530200 (2010CB530206) and the grants from the National Key Science and Technology Projects of China (No. 2009ZX10004-203 and 2008ZX10004-008). References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11090f1.jpg] [mb11090t1.jpg] |
| |||||||||
{kind=link}
{kind=link}