 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 379-382 Original Article Evaluation of the effect of presence of blood in the stomach on endoscopic diagnostic tests for Helicobacter pylori infection S Mittal, S Trakroo, V Kate, S Jagdish Department of Surgery, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry 605 006, India Date of Submission: 29-Apr-2011 Code Number: mb11092 PMID: 22120798 Abstract
Introduction: Presence of blood in the stomach has been thought to affect the performance of diagnostic tests used in detecting Helicobacter pylori (H. pylori) in the stomach. This study evaluated the effect of blood on the efficacy of rapid urease test (RUT) and microscopic appearance of the biopsy after staining with Giemsa stain. Keywords: gastro intestinal bleed, giemsa stain, Helicobacter. pylori, rapid urease test, tests for H. pylori Introduction H. pylori is a risk factor for peptic ulcer and other upper gastro intestinal (GI) disorders. [1] Diagnosis is by invasive techniques including rapid urease test (RUT), histological appearance of the mucosa when stained by Geimsa and culture. [2] Noninvasive tests including serology, urea breath and stool antigen test. [3],[4] Some reports have suggested that blood in the stomach decreases the sensitivity and specificity of RUT and histology [5],[6] while others have not shown any such decrease. [7],[8] One study showed an increase in RUT sensitivity. [9] This study was conducted to evaluate the effect of blood in the stomach on RUT and histology for detecting H. pylori as RUT and histology are the most commonly performed tests for the diagnosis of H. pylori in the gastroenterology suites. Materials and Methods This study was conducted prospectively in the department of surgery from July 2007 to June 2008. Two groups were studied:
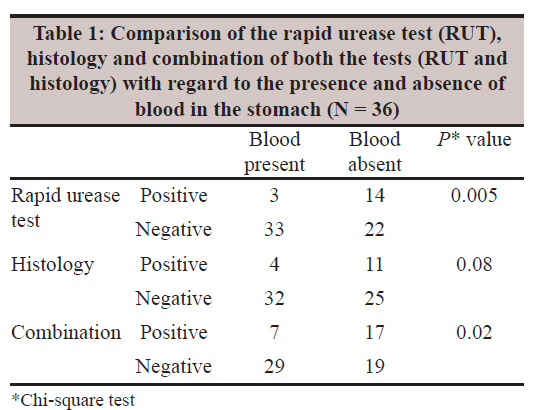
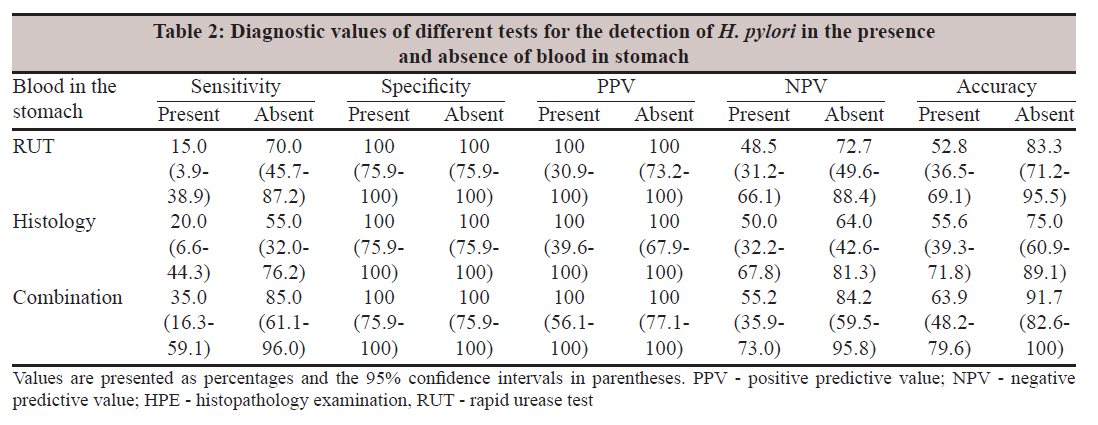
RUT was done using a standard technique. [10] The histology of the biopsy was studied after staining with Geimsa stain. Two endoscopic biopsies were taken from within 5 cm of the pylorus and processed for RUT and histology by Giemsa stain. The biopsies for histology were fixed in 10% formalin in the endoscopy room. [11] Paraffin embedded histological sections were stained with Giemsa for identification of H. pylori. A combined result of the two tests, RUT and histology, carried out in presence or absence of blood for the diagnosis of H. pylori, when taken together was considered as the gold standard. A positive H. pylori state was defined when either or both these tests were positive. When both the tests were negative, it was considered as a negative H. pylori state. What about the correlation with symptoms? Symptoms correlation was not done as many patients with bleeding oesophageal varices were asymptomatic except for the presence of bleeding which was not influenced by presence or absence of H. pylori. Patients were excluded from the study if they had received any form of anti-H. pylori therapy, or anti-secretory therapy in the preceding month or when patients were haemodynamically unstable, or had an international normalization ratio >1.5. Only patients who had come for index endoscopy and follow-up endoscopy were included in the study. Statistical analysis was done using Epi Info [TM] version 3.5 software. The comparison of RUT and histology for the detection of H. pylori in the presence and absence of blood in the stomach was done using the Chi-square test. Yate′s correction was done when deemed appropriate. Sensitivity and accuracy of these tests and their combination were determined. An alpha value of <5% was considered significant. The study was approved by the Institute Ethics Committee. Results A total of 36 patients with bleeding oesophageal varices according to the inclusion criteria were included in the study. There were 20 men and 16 women (M/F ratio = 1.25) with ages ranging between15 to 60 years (mean age = 44.14 years 2.1). The overall combination of tests at both the visits showed that 20/36 (55.6%) patients were positive for H. pylori infection. In the presence of blood in the stomach, RUT was positive in 3/36 (8.3%) patients where as histology was positive in 4/36 (11.1%) patients. In the absence of blood in the stomach, RUT was positive in 14/36 (38.9%) patients whereas histology was positive in 11/36 (30.6%) patients. Comparison of H. pylori positivity by RUT showed a significantly higher detection rate in the absence of blood in the stomach (8.3% vs. 38.9%; P=0.005). Comparison of H. pylori positivity for histology showed a higher detection rate in the absence of blood in the stomach. However this difference was not significant (11.1% vs. 30.6%; P=0.08). Furthermore, combination of these tests showed positive results in 7/36 (19.4%) in the presence of blood in the stomach, while in the absence of blood, it was positive in 17/36 (47.2%). This increase in positivity of the combination test in the absence of blood in the stomach was significant (19.4%. vs. 47.2%; P=0.02) [Table - 1] represents the positivity and negativity of RUT, histology and the combination of both the tests in the presence and absence of blood in the stomach. There was 55% decrease in sensitivity (70% vs. 15%) and 30% decrease in accuracy (83% vs. 53%) of RUT in presence of blood in stomach. How do you define it? Accuracy of RUT is defined as the number of true positives with true negatives determined by RUT alone when compared to the gold standard mentioned earlier. Similarly a decrease of 35% (55% vs. 20%) in sensitivity and 19% (75% vs. 56%) in accuracy was observed for histology in presence of blood in the stomach. The combination of these two tests showed decrease of 50% (85% vs. 35%) in sensitivity as well as 28% (92% vs. 64%) decrease in accuracy when blood was present in stomach. The values of sensitivity, specificity, positive and negative predictive value as well as accuracy of RUT, histology and combination of both these tests in the presence and absence of blood in the stomach are given in [Table - 2]. Discussion Sensitivity of RUT varies from 65% to nearly 100% in different studies. [12],[13],[14],[15] In patients with upper GI bleed, RUT gives more variable results. Several studies have reported low sensitivity of RUT (48% - 65%) in the presence of blood in the stomach. [16],[17] In our study, we found that the sensitivity of RUT was 15% in the presence of blood and 70% in the absence of blood in the stomach. Positivity of RUT significantly decreased in presence of blood in the stomach (P=0.005). A similar decrease in H. pylori detection rate of RUT was also reported by Leung et al. [5] They concluded that the presence of blood adversely affected the performance of RUT. This was due to the buffering effect of serum albumin on the pH indicator rather than a direct inhibition of urease activity. Houghton et al., reported lower detection rate of H. pylori with RUT. [18] They suggested that human plasma contained factors that killed H. pylori in vitro. On the contrary, several studies have excluded the role of blood in the stomach as a cause of false-negative results of RUT. For example, Perry et al., evaluated the in vitro effect of whole blood on RUT and concluded that false-negative test results in upper GI bleed could not be explained by the presence of whole blood. [9] Furthermore, Archimandritis et al., demonstrated that although RUT was unreliable for the detection of H. pylori infection in acute upper GI bleed, visible blood in the stomach did not influence results of the test. [17] Another study by Fernandez et al., in 2004 reported that in patients with blood in the stomach or an endoscopic sign of bleeding ulcer, the sensitivity of the RUT was almost 90% and this rate was higher than that found in patients without endoscopic signs of bleed (75.4%). [7] They concluded that the presence of blood in the stomach or endoscopic signs of bleed at the time of biopsy did not represent a conditioning factor for decreased sensitivity of RUT. Regarding histology, studies done earlier reported variable results. In this respect, some authors have reported a low sensitivity of histological tests in patients with upper GI bleed. Romero et al., described more false-negatives with histology in the upper GI bleed group than in the uncomplicated peptic ulcer group. [19] Colin et al., found sensitivity of histology as low as 33% in patients with upper GI bleed. [20] Similarly in our study we found sensitivity of histology was 20% in the presence of blood while it improved to 55% in the absence of blood in the stomach. We also found that positivity of histology improved from 11.1% in the presence to 30.6% in the absence of blood in the stomach. However, this difference was not significant (P=0.08). Other studies have shown histology to be more sensitive than RUT in diagnosing H. pylori infection in bleed ulcers. [16],[17] Finally, some authors have also demonstrated a high sensitivity of histology in patients with upper GI bleeding or have confirmed that visible blood in the stomach did not influence the accuracy of histological methods in diagnosing H. pylori infection. [17],[21] In addition to RUT and histology for detecting H. pylori, we have evaluated the combination of these two tests for sensitivity and accuracy. We found sensitivity of the combination was as low as 35% in presence of blood while it increased to 85% in the absence blood in the stomach. Similarly positivity of the combined test for the detection of H. pylori significantly improved from 19.4% in the presence of blood to 47.2% in the absence of blood in the stomach (P=0.02). References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11092t1.jpg] [mb11092t2.jpg] |
| |||||||||
{kind=link}
{kind=link}