 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
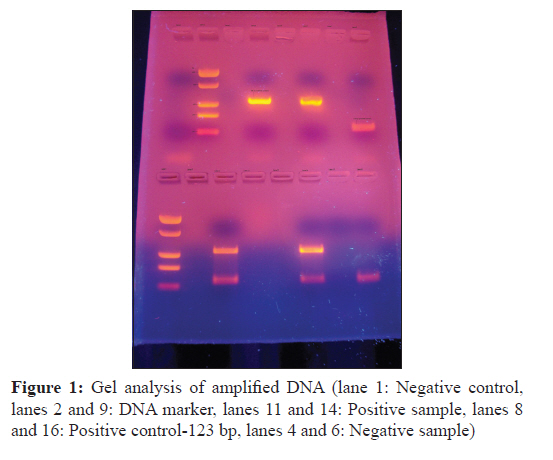
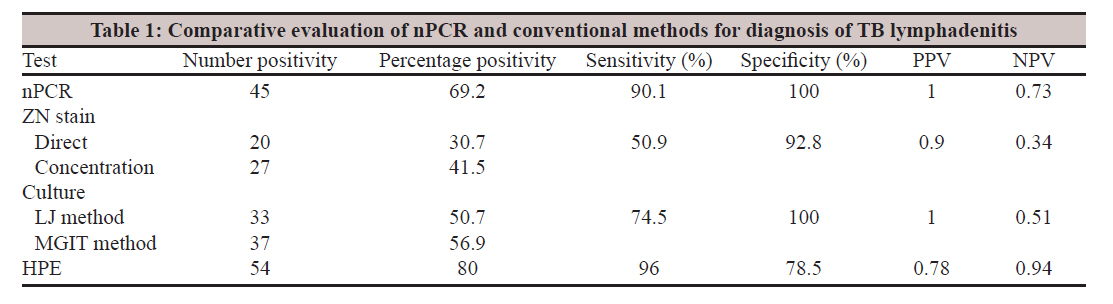
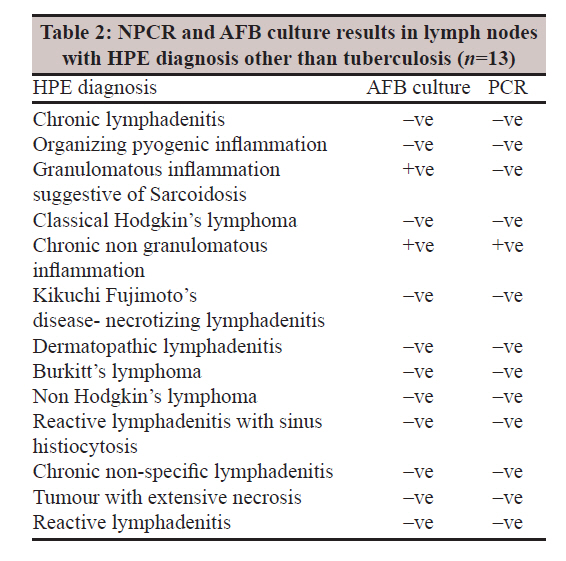
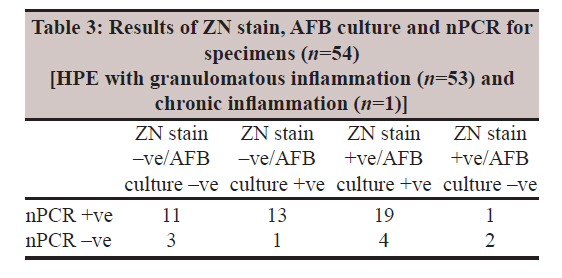
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 389-394 Original Article A study of tubercular lymphadenitis: A comparison of various laboratory diagnostic modalities with a special reference to tubercular polymerase chain reaction SA Patwardhan1, P Bhargava2, VM Bhide3, DS Kelkar4 1 Consultant Microbiologist, Deenanath Mangeshkar Hospital and Research Centre, Erandawane, Pune, India Date of Submission: 02-May-2011 Code Number: mb11094 PMID: 22120800 Abstract Objective: The purpose of our study was to compare various laboratory diagnostic methods, namely histopathological examination, Ziehl-Neelsen (ZN) stain, AFB culture by conventional Lowenstein-Jensen (LJ) method and fluorescence-based mycobacterial growth indicator tube (MGIT) technique and polymerase chain reaction (PCR) in clinically suspected cases of tubercular lymphadenitis. Keywords: Histopathology, mycobacterial growth indicator tube AFB culture, nested polymerase chain reaction, tubercular lymphadenitis Introduction Tuberculosis has been a major public health problem in India and continues to be so especially with high rates of HIV-TB co-infection. Lymph node tuberculosis constitutes about 20-40% of extra pulmonary tuberculosis. [1] It often presents as a challenge for clinicians when laboratory diagnostic tests fail to give conclusive evidence especially if bacteriological proof is lacking. The laboratory diagnosis of tubercular (TB) lymphadenitis is generally established by histopathology (HPE), microscopy for demonstration of acid fast bacilli (AFB) and mycobacterial culture on biopsy specimens. Each of these diagnostic methods has its own merits and demerits and varies in terms of sensitivity and specificity. The presence of caseation necrosis and epithelioid cell granulomas is taken as diagnostic of tuberculosis on HPE. However, granulomatous lymphadenopathy has a wide differential diagnosis and many other clinical conditions can present the same cytology and histopathology as TB lymphadenitis. Demonstration of AFB by Ziehl-Neelsen (ZN) stain is simple and rapid but lacks sensitivity. AFB culture is sensitive and highly specific but takes 4 to 12 weeks to give results with the drug susceptibility. Nucleic acid amplification techniques notably polymerase chain reaction (PCR) is being increasingly used to diagnose tuberculosis. This is largely due to the ability of PCR to increase the sensitivity, specificity and rapid turnaround time. However, even this technology has its own drawbacks, e.g. considerable demand in terms of technical expertise and inability to detect non tuberculous mycobacteria (NTM). A PCR laboratory was set up in our 450-bedded tertiary care hospital in Pune. We set up and validated a nested PCR (n PCR) test for M. tuberculosis. The aim of the present study was to compare the various diagnostic techniques, namely histopathology, microscopy by ZN stain, AFB culture by the conventional LJ method and fluorescence-based method using mycobacterial growth indicator tube (MGIT) technique and PCR in clinically suspected cases of tubercular lymphadenitis as regards sensitivity, specificity, rapidity, cost effectiveness and clinical utility. We also aimed to evaluate the utility of PCR in diagnosing TB lymphadenitis in our set up, especially when conventional methods like histopathology fail to give a definitive diagnosis. Materials and Methods This study was approved by institutional ethics committee. The study period was from August 2008 to February 2010. Study group A total of 65 paediatric and adult patients with lymphadenopathy clinically suspected to be of tuberculous aetiology were included in our study. The clinical symptoms suggestive of tuberculosis were fever and/or weight loss and lymph node enlargement. Informed written consent of all patients was taken for performing different diagnostic tests on the lymph node specimens. Sample collection Lymph node biopsies were divided into two halves; one half was collected in 10% formalin container for histopathological examination and other half was collected in a sterile container with sterile saline for AFB culture and PCR. Fine needle aspirates were not included in the study. Record of every patient as regards the demographic data, chief complaints, past history of tuberculosis, prior antitubercular treatment and HIV ELISA status was noted. Lymph node portion to be processed for PCR was stored at -20°C and for AFB culture at 4°C, maximum for 4 days. AFB culture Biopsy samples were homogenized in a sterile mortar and pestle and digested and decontaminated using the NALC (N-acetyl-l-cysteine) NAOH method. ZN stain was done on tissue smears directly after homogenization and after concentration as well. AFB culture was performed by the conventional LJ method as well as by fluorescence-based MGIT method (Becton Dickinson, Maryland, USA). The BD MGIT system is a rapid and reliable system for detection of mycobacterial growth and drug susceptibility. MGIT consists of a liquid broth medium, i.e. modified middle brook 7H 9 broth base which is enriched with OADC (oleic acid, albumin, dextrose and catalase) and added PANTA (polymixin B, amphotericin B, nalidixic acid, trimethoprim, azlocillin) to suppress contamination. In addition, the tube contains an oxygen-quenched flurochrome embedded in silicon at the bottom. During bacterial growth within the tube, free oxygen is utilized. With depletion of free oxygen, flurochrome is no longer inhibited resulting in fluorescence, intensity of which is directly proportional to extent of oxygen depletion and hence degree of growth. We use the semi-automated manual version of the MGIT system needing external incubation of the tubes at 37°C in a CO 2 incubator. 0.5 ml of concentrated specimen was inoculated into a MGIT vial and on to LJ medium. Growth was detected by daily monitoring of the tube with the help of the micro-MGIT reader to detect fluorescence. A growth index of more than 14 indicates mycobacterial growth. Mycobacterial growth shows granule formation in the medium. All positive MGIT vials were confirmed for the presence of acid fast bacilli by ZN staining. Positive vials were also subcultured on blood agar to rule out contamination before proceeding for sensitivity testing. Identification as M. tuberculosis or NTM was done on the basis of susceptibility of the isolate to PNBA (para nitro benzoic acid). The PNBA test was performed by the inoculating the positive culture into two MGIT tubes with and without PNBA (concentration of 500μg/ml per MGIT vial). The growth control tube (GC) was monitored for growth indicated by a growth index of more than 14. If the test strain was sensitive to PNBA indicated by no growth, it was identified as Mycobacterium tuberculosis complex. Growth of the test strain in the tube with PNBA indicated the presence of NTM. Quality control of the MGIT media and reagents used was carried out using standard H 37 RV and in-house strain of rapidly growing NTM, as well as negative control (distilled sterile water) for sterility check. Histopathology Formalin-fixed lymph node biopsy tissues were processed on an automated tissue processor, using 12 h cycle with 10% formalin, isopropyl alcohol, xylene and paraffin wax. A paraffin block of the processed tissue was made and sections were cut at 3 to 5μm thickness. They were stained with haematoxylin and eosin for HPE. Polymerase chain reaction All steps of PCR were performed in separate rooms to avoid carryover of templates. A commercially available PCR kit (Genei Tm , Bangalore Genei, Bangalore, India) was used. This test is a single-tube nested PCR. In the first step, the IS region of M. tuberculosis complex DNA sequence, a 220 bp, is amplified by specific external primers. In the second step, the nested primers are added to further amplify a 123-bp amplification product. DNA extraction All lymph node biopsies were homogenized in sterile mortar and pestle, diluted with 1 ml distilled water and centrifuged at 1000 rpm for 5 min. Supernatant was centrifuged at 10,000 rpm for 10 min and 250 ml of lysis buffer 1 and 20 ml of proteinase K were added to the resultant pellet. After mixing by vortexing, samples were incubated at 65°C for 30 min and then centrifuged at 10,000 rpm for 10 min. To 200μl of the supernatant, 200 ml of lysis buffer 2 containing internal control at the concentration of 10 ml/ml was added in a 2 ml eppendorf tube and incubated at 70°C for 10 min. Then, 200 ml of 96-100% ethanol was added and mixed by vortexing. This mixture was added to a spin column placed in a 2 ml collection tube and centrifuged at 8000 rpm for 4 min. The spin column was kept in a new 2 ml collection tube and washed twice with wash buffer provided in the kit and final centrifugation was performed at 14,000 rpm for 2 min. The flow through was discarded and the spin column given a spin at 14,000 rpm for 4 min. Then the spin columns were kept in 2 ml tubes and 100 ml of prewarmed (50°C) elution buffer provided in the kit was added. After incubating at room temperature for 5 min, it was centrifuged at 10,000 rpm for 3 min to elute the DNA. The DNA samples were preserved at -20°C for further processing. DNA amplification Two-step nested PCR was performed. The reaction profile for first amplification was denaturation at 94°C for 5 min followed by 20 cycles at 94°C for 30 s, 68°C for 1 min, 72°C for 1 min and a final extension at 72°C for 10 min. The reaction profile for second amplification was 94°C for 5 min followed by 30 cycles at 94°C for 30 s, 68°C for 30 s, 72°C for 30 s and final extension at 72°C for 7 min. Analysis of amplified products was done by electrophoresis on a 2% agarose gel containing ethidium bromide at 120 V for 30 min. Resultant bands were interpreted by UV transillumination. A product of 123 bp was indicative of the presence of M. tuberculosis. The internal control band was observed at 340 bp [Figure - 1]. Quality control was done by including a negative and positive control with every batch of samples processed. Results In our study, 65 (60 adult and 5 paediatric) patients with clinically suspected tuberculous lymphadenitis were included. 39 (60%) were females and 26 (40%) were males. Ages of patients ranged from 2 months to 76 years with a median age of 35 years. The biopsied lymph nodes included cervical in 29 (44.6%) followed by supraclavicular in 21 (32.3%), axillary in 12 (18.4%), abdominal in 2 (3.07%) and inguinal in 1 (1.53%). A majority of the lymph nodes received were right sided. 18/29, i.e. 62% of cervical; 15/21 i.e. 71.4% of supraclavicular and 8/12 i.e. 66.6% of axillary lymph nodes were right sided. 20 (30.7%) patients gave a history of receiving prior or being on antitubercular treatment. 17 patients (26.1%) in the study group were HIV infected. Culture by the MGIT method showed growth in 37 (56.9%) specimens, 36 of which grew M. tuberculosis and 1 grew M. fortuitum. In one sample, growth was obtained only on LJ medium in the eighth week of incubation. The mean turnaround time for culture positivity in ZN smear-positive specimens was 26 days on LJ and 13 days by the MGIT method. The same for the ZN smear-negative specimens was 30 days and 20 days by LJ and MGIT methods, respectively. AFB culture showed sensitivity of 74.5% and specificity of 100% [Table - 1]. In 13 (18.46%) specimens, the HPE gave a diagnosis other than tuberculosis [Table - 2]. Two of these patients were already on empirical antitubercular treatment for more than 1 month. PCR and culture were positive in one of these which was reported as ′chronic nongranulomatous inflammation′. One node which had the HPE diagnosis of ′granulomatous inflammation suggestive of sarcoidosis′ was culture positive for M. tuberculosis. Three ZN smear-positive specimens did not give positive culture results [Table - 3]. Two of these smear positive culture negative patients had already received antitubercular treatment 1 year back. Third smear positive, culture negative lymph node was PCR negative and was diagnosed as non-Hodgkin′s lymphoma on HPE. The false positive ZN stain result could have been due to contamination with NTM since the lymph node excision and collection was done in a private nursing home and the sample was sent to us for AFB culture. In 12 patients with HPE diagnosis of tuberculous inflammation, no growth was obtained on AFB culture and all of these were PCR positive [Table - 3]. All these patients were either on antitubercular treatment or gave history of antitubercular treatment with in previous 2 years. Histopathology results showed 96% sensitivity and 78.5% specificity [Table - 1]. In 53 lymph nodes reported histopathologically as ′granulomatous lymphadenitis′, the presence of epithelioid cells (52/53) and caseation necrosis (50/53) were the most common features noted. Langerhan′s type of giant cells was seen in only 38/53 lymph nodes. Of the 53 lymph nodes with HPE diagnosis of granulomatous lymphadenitis, 3 were smear negative and culture negative and PCR negative [Table - 3]. Two of these were reported as ′suggestive of tuberculous lymphadenitis to be correlated with microbiology results′ on the basis of ill-formed granulomas and small foci of non-caseating necrosis. Both these patients were on empirical anti-tubercular treatment for 3-4 months and complained of persistent fever and lymphadenopathy indicating the aetiology to be probably non-tubercular. The third lymph node showed all classic histopathological features of tuberculosis. The patient was a 2 month old baby with generalized lymphadenopathy. The histopathologists reviewed the HP slides on request of the treating clinician. The HPE diagnosis was later on given as ′Langerhan′s cell histiocytosis′ after immunohistochemical staining (Langerhan′s cell histocytes S-100 positive as against histiocytes encountered in TB which are S-100 negative). Sixteen out of 17 HIV positive patients had histopathology diagnosis of tuberculous inflammation. Epithelioid cells (15/16) and caseation necrosis (16/16) were the most frequent HP changes noted. Langhan′s giant cells were seen only in 9 of the 16 nodes. In 9 of the 16 patients (56.25%), granulomas were conspicuously absent or ill formed. Culture grew M. tuberculosis in 15 of these patients and M. fortuitum in 1. PCR was positive in all except for the patient with M. fortuitum. Amongst the 54 lymph nodes with HPE suggestive of TB lymphadenitis, correlating TB PCR results with various histopathological features revealed that PCR negativity (9/54) was seen only in the presence of granulomas. Lymph nodes showing chronic inflammatory changes or only caseation necrosis were not associated with negative PCR results. The overall PCR positivity in these 65 cases was 69.2% (45/65). The sensitivity and specificity of PCR were 90.1% and 100%, respectively [Table - 1]. There were five specimens where PCR was negative in spite of culture positivity [Table - 3]. In one of these, the PCR result was true negative explained by growth of M. fortuitum on culture. In the other four, PCR negativity was unexpected. PCR was negative in two specimens which were ZN smear positive and culture negative [Table - 3]. In one of these, PCR was a true negative since the presence of AFB in the ZN smear was possibly due to contamination of the specimen with NTM as mentioned earlier. Discussion In our study, which included lymph node specimens from 65 patients with clinical diagnosis of TB lymphadenitis, PCR proved highly sensitive (90.1%) and specific (100%) test. The positive predictive value and negative predictive value of PCR was 1% and 0.73% respectively. We used nested PCR for the M. tuberculosis IS6110 sequence which is present in high copy numbers in most strains of M. tuberculosis complex and hence is a good target for getting diagnostic specificity. In addition, using the nested PCR technique makes the test more sensitive than one step PCR. In a study, comparing two different targets, namely IS6110 element and 65 kDa antigen for PCR assay on lymph node tissues, the IS6110 PCR had higher sensitivity (89%) compared to 65 kDa (6%). [2] A sensitivity of 68% and specificity of 86% were reported for TB PCR done on lymph node biopsies in a study comparing PCR with conventional techniques for detection of M. tuberculosis in granulomatous lymphadenopathy. [3] However, in this study a single step dev R-based PCR was used. A study comparing IS6110 nPCR with various histopathologic features in TB lymphadenitis reported 78% sensitivity and 88% specificity for PCR. [4] A recent study in Mexican children, evaluating an IS6110 based nPCR for diagnosis of cervical lymphadenitis noted a sensitivity of 96% and specificity of 93%. [5] In our study, PCR was positive in 24 (44.4%) smear negative lymph nodes. This ability of PCR to detect M. tuberculosis in smear negative specimens is remarkable for giving a definitive and rapid diagnosis especially with possible false positivity of HPE diagnosis or at times when HPE results are inconclusive. This helps in reducing the need of any further invasive diagnostic procedures. PCR was false negative in four patients where culture grew M. tuberculosis. This false negativity could have been due to sampling errors, inefficient extraction of DNA or the presence of PCR inhibitors in specimens. This could also be due to the absence of the IS6110 in these M. tuberculosis strains as has been reported in some studies. [6] In one of these false negative specimens, a repeat PCR was positive after 1 in 10 dilution of the lymph node sample. This was done to dilute the PCR inhibitors in the specimen as has been reported by Tyagi et al. [3] However, we could not repeat the test after dilution in other three patients as there was no residual specimen. In 12 patients, culture was negative and PCR was positive. All of these patients were receiving antitubercular treatment and PCR positivity indicated the presence of M. tuberculosis DNA in the specimens. AFB culture positivity in our study was 56.9% with a sensitivity of 74.5% and specificity of 100%. Tyagi et al. have reported culture positivity of 14% and sensitivity of 23% in their study comparing conventional techniques and PCR for detection of M. tuberculosis DNA in granulomatous lymphadenopathy. [3] In a similar comparative study by Das et al., positivity of 22% was reported for culture. [7] A recent study on cervical tuberculous lymphadenitis in Mexican children, 26% AFB culture positivity was noted. [5] All these studies however used LJ media for culture. Use of liquid medium-based culture could have resulted in increased yield. We found the MGIT method to be superior to LJ culture both in terms of positivity and time to positivity. Rodrigues et al. have also highlighted this in their study on evaluation of MGIT 960 system. [8] They reported an average detection time of 16 days for smear negative specimens and 13.2 days for paucibacillary extra pulmonary specimens similar to that in our study, i.e. 20 days and 13 days, respectively. In our study, one specimen which showed growth on LJ medium at the end of 8 weeks highlights the importance of simultaneous LJ culture and incubation of these slopes for at least 10-12 weeks. We have isolated till date (including one in the present study) eight NTM from lymph node specimens. Four of these were HIV-negative healthy adults. 5/8 (62%) of these NTM belonged to the rapid growers group. Few other workers have also reported NTM lymphadenitis occurring in healthy adults and rapid growers being the most frequent isolates. [10],[11] Histopathology shows a compromised specificity (78.5%) in our study. Isolation of M. tuberculosis from the specimen with HPE diagnosis of sarcoidosis was noteworthy. Earlier workers also have noted TB lymphadenitis presenting as sarcoid-like granulomas or demonstration of M. tuberculosis in tissues affected by sarcoidosis. [12],[13] Poorly formed granulomas were significantly more commonly seen in HIV positive patients (56%) as compared to HIV-negative patients (22.9%), which could be attributed to immunodeficiency. In our experience, PCR can be effectively used to achieve a maximum sensitivity in early and rapid diagnosis of TB lymphadenitis particularly in light of possible false positive or inconclusive histopathology results. A positive PCR result to support HPE finding of ′granulomatous inflammation suggestive of tuberculosis′ increases its positive-predictive value. However, as PCR detects both live and dead bacilli, its positivity should be seen in light of the overall clinical picture especially in patients receiving anti tubercular treatment. Acknowledgement
References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11094t3.jpg] [mb11094f1.jpg] [mb11094t2.jpg] [mb11094t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}