 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 395-400 Original Article Opportunistic infections in relation to antiretroviral status among AIDS patients from south India S Srirangaraj1, D Venkatesha2 1 Department of Microbiology, Mahatma Gandhi Medical College and Research Institute, Pondicherry 607 402, India Date of Submission: 08-Dec-2010 Code Number: mb11095 PMID: 22120801 Abstract Background: There is a need to generate data from India on relative frequencies of specific opportunistic infections (OIs) in different regions and their relation to the choice of commonly used generic highly active anti-retroviral therapy (HAART) regimens. Keywords: Anti retroviral therapy regimens, highly active anti-retroviral therapy, opportunistic infection, tuberculosis Introduction Opportunistic infections (OIs) are a common complication of HIV infection. OIs cause substantial morbidity and hospitalisation, necessitate toxic and expensive therapies and shorten the survival of people with HIV infection. With a high disease burden of 2 million to 3.1 million in India, [1] it is imperative to know the relative frequencies of specific OIs in different regions of the country, so that appropriate management strategies can be devised to counter them based on these data. Though there are well-documented studies from the western world and Africa, [2],[3],[4] the number of studies from India on this aspect are comparatively lesser. [5],[6] We, therefore, conducted this prospective observational cohort study to document the prevailing prevalence pattern of OIs both before and after highly active anti-retroviral therapy (HAART) initiation in a south Indian state. The other objectives of this study were to assess the risk of developing an OI after HAART initiation and also to see if there was any difference in the risk of developing an OI in the first year after HAART initiation, for those on Efavirenz- based regimens when compared with those on Nevirapine-based regimens (as these are the commonly used regimens under the National AIDS Control Program). Materials and Methods A prospective observational cohort study was conducted, involving 108 randomly selected newly registered ART (anti retroviral therapy)-naοve HIV positive patients, attending our ART Centre, from August 20, 2006 onwards. The duration of study period was 1 year from August 20, 2006 to August 19, 2007. The study was approved by the ethical review board of the institute and a written informed consent was obtained from all the participating patients. After taking an informed consent (for HIV testing), these 108 individuals, voluntarily attending our Integrated Counselling and Testing Centre (ICTC) at the Department of Microbiology, underwent pre-test counselling by male or female ICTC counsellors, followed by HIV testing as per the strategy III of the NACO (National AIDS Control Organization) guidelines (for HIV testing). [7] After they were identified as HIV-positive, post-test counselling was given, and they were referred to the ART Centre in our hospital, where they underwent pre-ART counselling. After clinical evaluation, informed consent was taken from these patients and they were enrolled into the study after they satisfied the inclusion criteria. They were then started on HAART as per the World Health Organization (WHO) guidelines. [8] All the 108 individuals selected in this cohort were eligible for ART and had satisfied the following inclusion criteria:
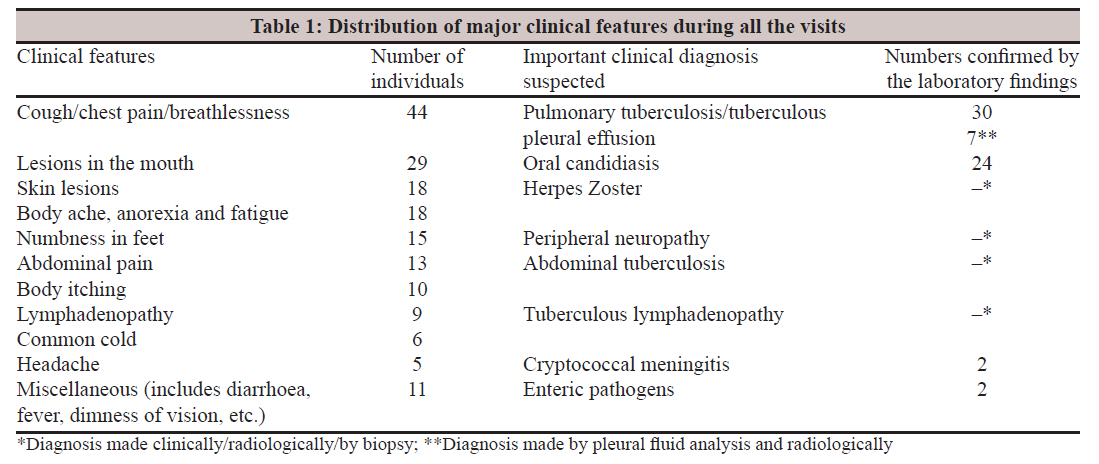
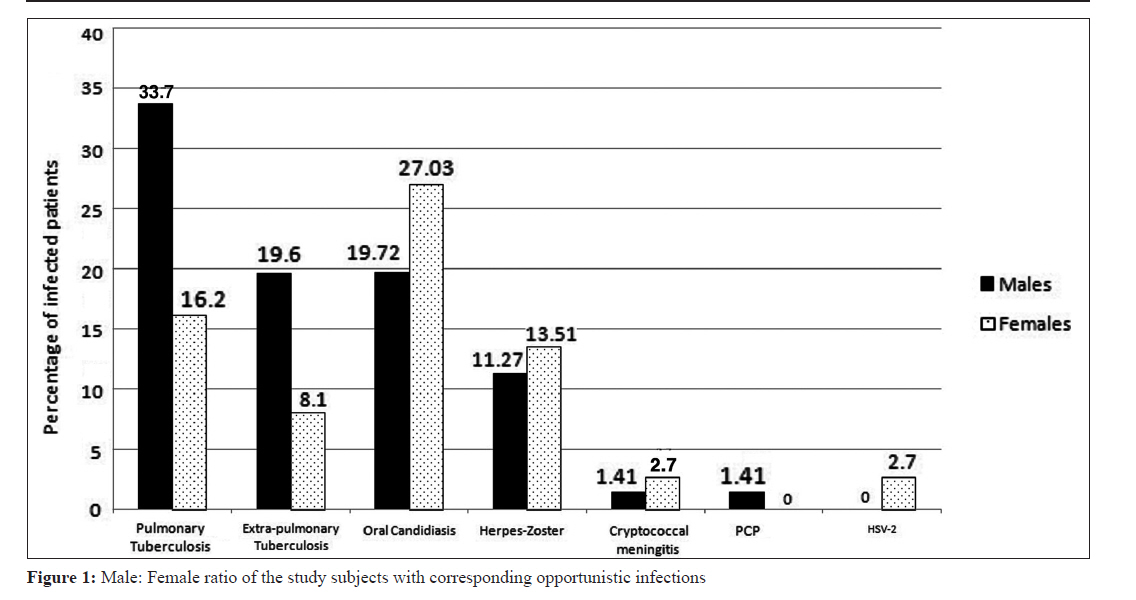
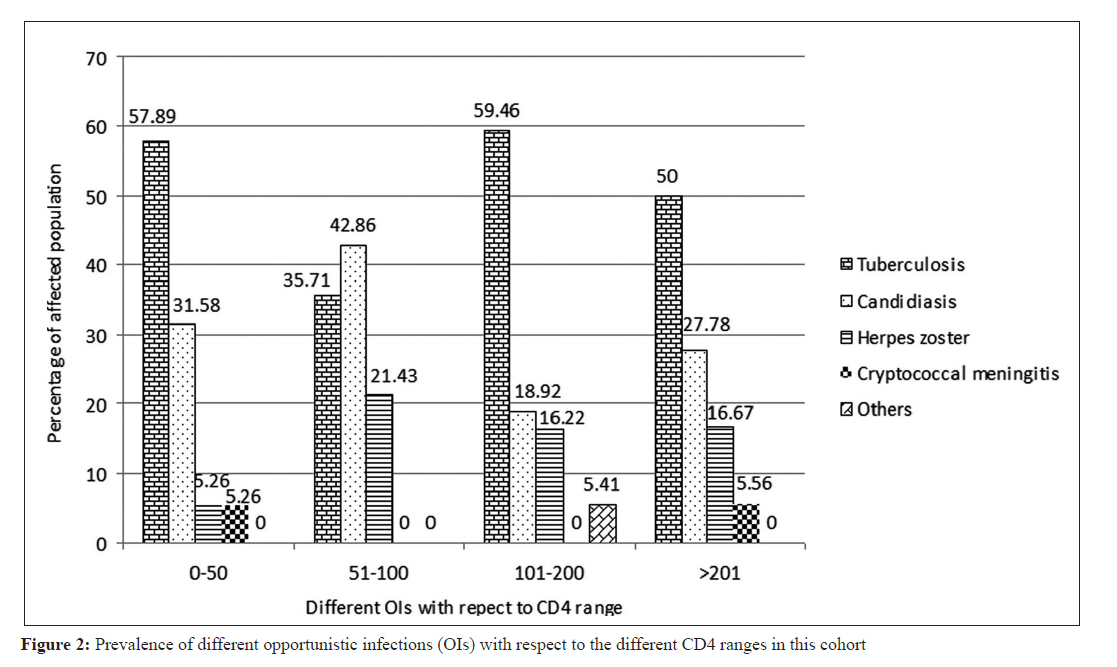
The exclusion criteria were HIV-seronegative individuals and those on prior ART were excluded. CD4/CD3 enumeration The CD4/CD3 enumeration was done using the single-platform BD FACS Calibur TM machine (Becton, Dickinson and Company, San Jose, United States of America), by strictly following the manufacturer′s instructions. [9] For each patient, the clinic visit prior to initiating a new HAART regimen served as the baseline, during which the CD4 counts were recorded. After initiation of HAART, these patients were followed up at regular intervals of every 3 months until the end of the study period. At the initial visit, they were interviewed to fill up the pre-structured questionnaire. Then, depending on the patient′s clinical features, specimens were collected which included stool, sputum (three sputa specimen - first spot, early morning and second spot) and oral swab. All the three sputum samples were used to make separate smears and stained by Ziehl-Neelsen method. Diagnosis of tuberculosis was made by strictly following the Revised National tuberculosis Control Programme (RNTCP) guidelines. [10] Stool specimens were collected according to the WHO standard procedures and examined microscopically using saline wet mounts. Lugol′s Iodine was used for the detection of ova, larvae, trophozoites and cysts of intestinal parasites. Smears of direct specimens were examined by modified acid fast staining for Cryptosporidium parvum, Isospora belli and Cyclospora. [11] Also, bacteriological culture of the stool specimens was done following the WHO standard procedures to mainly identify Salmonella and Shigella. [12] For the diagnosis of Candidiasis, oral swab specimen was cultured on to Sabouraud′s dextrose agar (SDA) and the suspected colonies were identified by the germ tube test following standard microbiological procedures. [13] Diagnosis of cryptococcal meningitis was made by India - ink preparation of the Cerebro Spinal Fluid (CSF) and by culture on SDA. Hepatitis B virus (HBV) infection was detected by ELISA using HEPALISA HBsAg kit (M/S J. Mitra and Co. Ltd., New Delhi, India), by strictly following the manufacturer′s instructions. However, diagnosis of Herpes Zoster, Pneumocystis jiroveci pneumonia and Herpes genitalis were made only clinically. These procedures were followed on each subsequent visit till the end of the study period. The diagnosis of cerebral toxoplasmosis was done at the National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore, where the patient was referred. Data entry, database management and analysis were done with use of SPSS software (version 16.0, SPSS, Chicago, IL, USA). Descriptive statistics were used to calculate the frequency, mean, percentage and standard deviation. The incidence of opportunistic infections (OIs) was estimated using cumulative incidence estimates. Statistical comparison for time-to-event data to calculate the risk of developing an OI after HAART initiation and also to assess the difference in the risk of developing an OI for those on different ART regimens was performed using the likelihood ratio test from Cox regression models. All reported P values are two-sided and P<0.05 was considered statistically significant. Results In this study, 108 HIV patients with OI were studied, of whom, 71 (65.74%) were males and 37 (34.26%) were females. The majority 53 (57.24%) of patients were 31-40 years old followed by 36 (38.88%) patients and 19 (20.52%) patients in the age groups 21-30 and 41-50 years, respectively. The distribution of the study population according to CD4 cell count/cu.mm of blood was a maximum of 41.7% (45 cases) of the population with 101-200 CD4 cell count, followed by 21.30% (23 cases), 18.5 (20 cases) and 18.5% (20 cases) of patients with ≥201, 51-100 and ≤50 CD4 cell counts, respectively. Most of them 70 (64.8%) were from a rural background, a significant proportion of them 56 (51.85%) were illiterate or primary school educated. Seventy-four (68.6%) of them were married and the predominant mode of transmission of HIV was by heterosexual transmission, accounting for 90 (83.4%) of cases. [Table - 1] shows the distribution of major clinical features in this cohort during all the visits. Cough/chest pain/breathlessness was the commonest presenting clinical features in our patients. Before HAART initiation, among the spectrum of OIs observed, Tuberculosis emerged as the most frequent infection, developing in 47 (53.4%) of the patients. Oral Candidiasis emerged as the second most prevalent infection, developing in 24 (27.2%) subjects. Herpes Zoster seen in 13 (14.7%) of patients was the third most prevalent infection, followed by Cryptococcal meningitis seen in 2 (2.7%) cases and 1 case each (1.1%) of Pneumocystis jiroveci pneumonia and Herpes genitalis. Fourteen (18.92%) of these patients had dual OIs and two (1.9%) patients were co-infected with HBV. Majority of the patients (79.55%) with OIs had CD4 counts ≤200 cells/ml. A significant proportion 74 (68.52%) of the study subjects had at least a single OI before initiation of HAART. Of the total number of patients with tuberculosis (n=47), 63.83% (30 cases) had pulmonary tuberculosis, 14.89% (7 cases) had tuberculous pleural effusion, 10.64% (5 cases) had tuberculous lymphadenitis, 8.51% (4 cases) had abdominal tuberculosis and 2.13% (1 case) had tuberculous meningitis. The distribution of different OIs according to the male: female ratio is shown in [Figure - 1]. A very high proportion of males suffered from Tuberculosis (53.52%) when compared with females (24.32%). However, the proportion of females suffering from oral Candidiasis, Herpes Zoster and Cryptococcal meningitis was higher when compared to males. The prevalence of different OIs relative to the CD4 cell count of the study population is shown in [Figure - 2]. This shows that Tuberculosis is the most important infection in all the CD4 ranges. The number of total OI events dropped down to just 9 (8.26%) cases after HAART, of which 6 were new OI events and 3 were old OI events, i.e., those which continued to persist despite ART. There was a drastic reduction of 96.59% in OI events after 6 months of HAART from a total of 88 OI events recorded (from 74 of the 108 subjects in this cohort) before ART to only 3 events of old OI recorded after ART. The risk of development of a new OI after HAART initiation in this cohort was 5.56%. The new OIs developed after ART were Herpes Zoster seen in 1 case, non-typhoidal Salmonellae in 1 case, cerebral Toxoplasmosis in 1 case, oral Candidiasis in 2 cases and 1 case of cryptosporidiosis. Of these, one case had dual OIs. The time for the development of an OI in the first year of therapy tended to be shorter for the NVP-based regimens than with EFV-based regimens, but this difference was not statistically significant (HR=0.891, 95% CI: 0.179-4.429; P=0.888, not significant). For those who initiated therapy, CD4 count of <100 cells/cu.mm or <200 cells/cu.mm was not a significant factor in developing an OI in the first year after HAART whether they were on NVP-based regimen or on EFV-based regimen (P=0.176 for CD4 count <100cells/cu.mm, Hazard ratio (HR)=4.258 and P=0.993 for CD4 count <200 cells/cu.mm, HR=1.007). Discussion In our study, the age group of 31-40 years (57.24%) continues to be the most commonly involved age group as has been seen in studies from India and abroad. [6],[14],[15],[16],[17] As HIV affects the economically productive age groups, the overall economic burden on the country is increased. The major mode of HIV transmission in this study was heterosexual contact, found in 83.4% of cases. Thus, heterosexual contact continues to be the most important means of acquiring HIV in India, as was identified in earlier studies from India. [6],[16] The lower median CD4 count of 124 cells/cu.mm in our study may be on account of late detection of the infections due to inadequate laboratory facilities at the peripheral health centres, where treatment may be held up until significant immunosuppression has already set in, at which point patients are referred to tertiary care hospitals. Another important observation in the present study was that 68.52% of the study subjects were suffering from at least a single OI before initiation of HAART. This high OI burden could be partly secondary to associated malnutrition, overcrowding, poor hygiene and lack of a good public health infra-structure as suggested by Raviglione et al.[18] The high prevalence rate may also be due to the fact that this study was conducted at a major tertiary-care government hospital where patients seeking care are mostly referred from peripheral health care centres. A greater prevalence of OIs was observed in those with CD4 counts below 200 cells/cu.mm, which is a well documented finding. A high prevalence (45%) of Tuberculosis infection was found in our investigation. Similar findings were reported from Chennai. [6] Extra pulmonary form was seen in 36.17% of the TB patients in our study. A high burden of extra pulmonary TB was also reported from Bangalore. [19] This finding shows that Tuberculosis is one of the most common OIs in AIDS patients in India. This also underlines the need to institute appropriate TB control measures on a massive scale all over India. Furthermore, special emphasis should be given for the screening of tuberculosis for those patients with CD4 counts less than 200. However, in contrast to these findings, studies from Nepal have documented lower prevalence rates of Tuberculosis in HIV seropositive patients, ranging from 10% to 23%. [14],[17],[20] These findings illustrate the difference in prevalence patterns in different geographical locations and further bolster the case for devising region-specific strategies to counter OIs based on the local prevalence pattern. Similar to a study by Sharma et al., [14] we observed in our study that except for Tuberculosis and candidiasis, there was no regular trend observed in the prevalence of other OIs with respect to CD4 counts. This might be on account of the Cotrimoxazole prophylaxis taken by all our patients irrespective of their CD4 counts, which might have prevented or influenced the occurrence of other OIs. This also explains the lower prevalence of enteric opportunistic pathogens such as Salmonella spp and Isospora belli in our study. Drastic reduction in OI events after 6 months of HAART observed in this study is also a well-documented finding. [5],[15] Nevirapine and Efavirenz-based regimens are the commonly used regimens in the NACP (National AIDS Control Programmed) in India. Our finding that there was no statistically significant difference in the risk of developing an OI between the EFV-based and NVP-based regimens, indicates that both the regimens are equally efficacious in controlling OIs and the choice of the regimen will not be a risk factor in event of an OI event occurring after HAART initiation. Though the short duration of the study period and the small sample size of the cohort are the major limitations of this study, we believe the results obtained here will help provide information that can form the basis for more elaborate and systematic studies on this subject in the future and will directly impact patient care by tailoring the prophylaxis needs for OI prevention according to the prevailing OI prevalence pattern in a particular region. Acknowledgements The authors want to acknowledge Mr. Khan Ghori for his technical support and Dr. Noyal Maria Joseph for his help with statistics. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11095t1.jpg] [mb11095f2.jpg] [mb11095f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}