 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 406-410 Original Article Standardization of fungal polymerase chain reaction for the early diagnosis of invasive fungal infection P Deshpande1, A Shetty2, A Mehta2, F Kapadia3, A Hedge3, R Soman3, C Rodrigues4 1 Department of Research, PD Hinduja National Hospital and Medical Research Centre, Veer Savarkar Marg, Mahim, Mumbai 400 016, Maharashtra, India Date of Submission: 18-Oct-2010 Code Number: mb11097 PMID: 22120803 Abstract
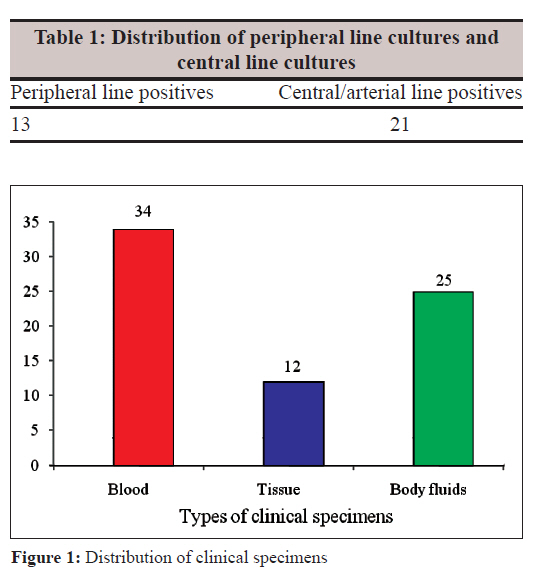
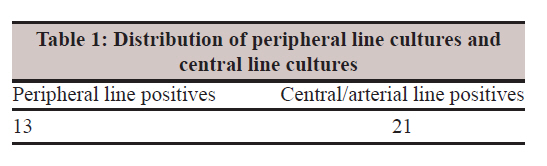
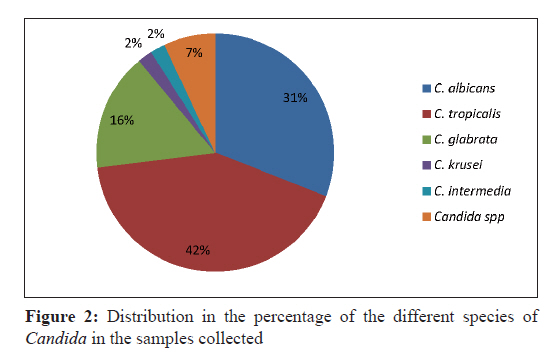
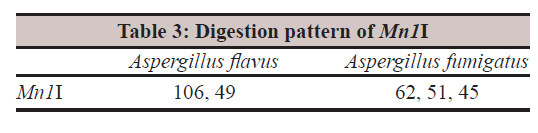
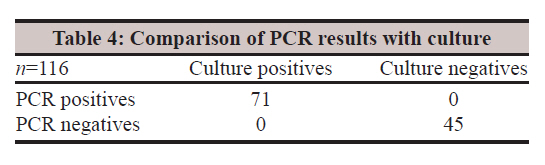
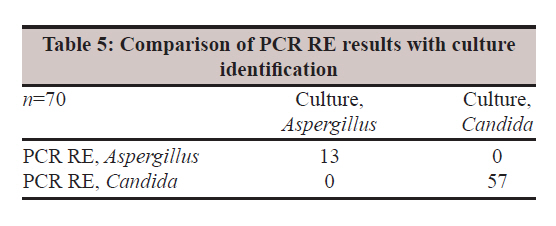
Background: An early initiation of antifungal therapy in invasive fungal infections (IFIs) is critical in reducing the high mortality rate. Current diagnosis of fungal infection relies on microscopy, culture, antigen, antibody specific tests and histological diagnosis. However, these tests either lack sensitivity or specificity. There is thus the need for a rapid, specific and accurate diagnostic method. Keywords: Aspergillus, Candida, nested polymerase chain reaction, polymerase chain reaction, restriction enzyme digestion Introduction The prevalence of invasive fungal infections (IFIs) has increased due to an increasing population of immunocompromised patients, intensive immun-osuppressive chemotherapy, increasing awareness of fungal infections and the widespread use of broad-spectrum antibiotics and invasive devices. [1] Compared with bacterial infections, IFIs occur less frequently; however, the infection-associated morbidity and lethality are significantly higher than bacterial infections. Invasive candidiasis (IC) and invasive aspergillosis (IA) account for 15-20% of the prevalence in patients at high risk. In tertiary care practice, the most common fungal pathogens are Candida and Aspergillus species accounting for more than 90% of mycoses. [2] A tertiary care hospital in North India showed an 11-fold increase in cases with candidaemia in the second half of the 1980s and a further eighteen fold rise from 1991 to 1995. Candidaemia is now the fourth most common cause of bloodstream infection at that institute, most of those cases being reported from ICUs. [3] Recent epidemiologic trends indicate a shift towards non-Candida albican infections. Culture is the ′gold standard′ for the detection of fungal infections but this is believed to lack sensitivity and has been shown to be positive in less than 50% of patients with IC and rarely positive in patients with IA. Galactomannan and β-d-glucan have limited specificity and sensitivity due to variable cut-off values, performances in different sample matrices and antigen variability. Diagnosis by biopsy or histopathology is difficult due to the severity of illness in immunocompromised patients. Hence there is a need for a rapid, specific and accurate diagnostic method. Different molecular methods like PCR have been developed for the early detection but have drawbacks regarding their sensitivity. Our aim was to establish a new, highly sensitive, and specific PCR for the rapid detection of Candida and Aspergillus species in blood, body fluids and tissue specimens. Materials and Methods Setting The study design and protocols were approved by the Ethical Research Committee of the P. D. Hinduja National Hospital, and Medical Research Centre, Mumbai, Maharashtra, India, where this study was conducted. The study involved indoor patients admitted from 2007 to 2009. Reference fungal strains C. albicans ATCC 10231, Candida tropicalis ATCC 66029, Candida krusei ATCC 14243, Candida kefyr ATCC 66028, Aspergillus fumigatus ATCC 13073, Aspergillus flavus ATCC 16883 and Aspergillus niger ATCC 16888 strains were used for the standardization of DNA extraction and for nested PCR. These strains were subcultured on blood agar, Sabouraud′s agar and CHROM agar plates. Fungal strain preservation All ATCC fungal strains and the strains obtained from clinical samples were subcultured twice into Sabouraud agar and stored at −80°C. The strains were also streaked on Sabouraud agar slants and were stored at 4°C for continuous subculturing purposes. Clinical sample collection Consecutive culture proven samples of IFIs were collected as per the definitions/criteria given by European Organization of Research and Treatment of Cancer (EORTC). Only samples which were culture positive were selected for the standardization of the fungal PCR. Inclusion criteria Sterile site clinical specimens were collected, i.e., tissue specimens, blood and body fluids like peritoneal fluid/CSF since IFIs are deep-seated infections. Exclusion criteria Non-sterile samples like BAL, cranial sinus cavity, urine and stool were excluded. Controls A total of 45 negative controls included the following: 15 healthy controls (absence of infection), 30 diseased controls in which 15 were samples from patients suffering from bacterial sepsis (blood culture positive) and responding to antibacterial agents and 15 samples from patients with documented HBV and HIV infection. Clinical sample preservation All clinical specimens and controls were stored at −80°C until DNA extraction. DNA was extracted using the QIAamp DNA Mini kit and stored at 80°C. DNA extraction The extraction of the ATCC fungal strains and clinical specimens was performed using the QIAamp DNA Mini kit. The heat shock method was incorporated in the existing Qiagen protocol for effective lysis. The samples were incubated at 100°C in water bath for 3 min and then transferred to liquid nitrogen (−196°C) for 1 min. The cycle was repeated three times and the temperature difference led to the disruption of the fungal cell wall. The DNA extraction protocol was standardized using reference fungal strains and blood spiked with the desired fungal load (10 6 -10 CFU/ml). Molecular analysis Nested PCR was performed on extracted DNA. PCR was initially standardized using standard Candida and Aspergillus strains. The optimized conditions were later performed on clinical samples. 18S rRNA was used as the target gene since it contains highly conserved sequences. Four PCRs were standardized in total: Two for Candida species and two for Aspergillus species. All lyophilized primers were reconstituted using a Χ1 Tris EDTA buffer so as to obtain a 100 pmol/μl stock solution. A working stock solution of 10 pmol/μl was subsequently prepared using a 10 mM Tris chloride buffer. The primers used for Round I of Candida and Aspergillus were as follows: F1-5'ATT GGA GGG CAA GTC TGG TG 3′ and R1-5′CCG ATC CCT AGT CGG CAT AG 3′. These primers were published primers described by White et al. Internal control, i.e., beta globin ( house keeping gene) was added in Round I of both the nested PCRs to check for PCR inhibition, the primers being as follows: BGF-5′ TGA ACG TGG ATG AAG TTG GTG GTG 3′ and BGR-5′ACT TTC TTG CCA TGA GCC TTC ACC TT 3′. For all the PCR experiments in this study, the Eppendorf Master Gradient Thermal Cycler has been used. All PCR experiments have been carried out using 50μl reaction volumes in 0.5-ml PCR vials. Round I PCR was performed in a total volume of 50 μl PCR reaction mixture containing 20 pmol of the primers, 100 mm dNTPs, 2 mM MgCl 2 and 1.5 units of Taq polymerase (1 unit/μl). PCR products of Round I (0.2μl) of the nested PCR were used as the template for Round II. Primers were designed for Round II to target both Candida and Aspergillus species and they were as follows: F2-5′ GCTC GTA GTT GAA CCT TGGG 3′ and R2-5′ GCCT GCT TTG AAC ACT CTAAT 3′. This PCR reaction mixture, too, contained 20 pmol of Round II primers, 100 mm dNTPs but had 2.5 mM of MgCl 2 and 0.5 U Hot Star Taq polymerase. The primers amplified a product of approximately 150 bp (depending on the species). All the products were checked on the 4% agarose gel. Round II products were subjected to restriction enzyme digestion. For the Candida species, restriction enzymes used were BSeYI and Hpy188I while for the Aspergillus species, Mn1I was used. The digested products were analyzed by 4% agarose gel electrophoresis for identification. PCR validation Analytical sensitivity Blood from healthy individual was spiked with the desired fungal load (10 6 -10 CFU/ml) to standardize DNA extraction and to detect the analytical sensitivity of the PCR. Serial dilutions were prepared in a fungal saline using reference Candida strains (0.5 McFarland suspension, ~10 6 CFU/ml). Healthy blood samples were spiked with each of these dilutions (10 6 -10 CFU/ml). Primer specificity The primers were tested for their ability to identify their correct target organism. The specificity of the primers was checked against Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Mycobacterium species, Cryptococcus neoformans and human genomic DNA. The primers were found to be highly specific and did not amplify any other organisms. Quality control Blood from healthy individuals and molecular grade water were included as negative controls. For each PCR the following controls were included: (a) extraction controls (positive and negative), (b) positive PCR controls (DNA from cultures fungal strains), (c) internal control - beta globin (added in Round I) and (d) negative controls for Rounds I and II. PCR validation was performed by sequencing. The representative sequencing of Rounds and II products (of each species) was also performed. A BLAST search was done to verify that the intended target was amplified. All the sequenced amplicons showed 99% homology with the respective culture isolates. Precautions taken to avoid cross contamination Dedicated pipettes, aerosol barrier filter tips and molecular grade reagents were used for extraction and PCR amplification. A unidirectional work flow was followed. The extraction of DNA, preparation of master mix, addition of template and amplification were carried out in biosafety hoods in separate laboratories that were independently equipped. All work surfaces were wiped with 5% hypochlorite and 70% ethanol at every stage. Results In a period of 2 years, 71 culture proven cases of IFIs were collected. All suspected specimens, which were also sent for fungal culture, were stored. Only samples that were culture positives were processed. The distribution of clinical specimens is shown in [Figure - 1]. Only sterile site cultures were collected to rule out the possibility of colonization since IFIs are deep-seated infections . Samples were collected concurrently with those taken for culture before the initiation of antifungal therapy. Whole blood samples were collected from immunocompromised patients to target both free DNA and intracellular DNA. The majority of samples were blood samples followed by body fluids and tissue specimens. A total of 70.4% of the samples were obtained from the intensive care setting. Among the blood samples (n=34), peripheral line cultures were considered to be true cases of candidaemia as compared to the central and arterial line cultures [Table - 1]. This was performed to rule out the possibility of colonization in the invasive devices of these line cultures. Of the 71 culture positives, 57 were positive for Candida, 13 were growing Aspergillus species and 1 sample was positive for Trichosporon asahii. The distribution in the percentage of the different species of Candida in the samples collected is shown in [Figure - 2]. Among the Aspergillus species, A. fumigatus (n=10) was the most predominant organism followed by A. flavus (n=3). All negative controls were negative by the fungal nested PCR. Fungal DNA extraction was performed on all the 71 clinical specimens and the 3 control groups. The standardized nested PCR was applied to the spiked blood samples and the serially diluted Aspergillus DNA. This was done to check the analytical sensitivity of the fungal nested PCR. The analytical sensitivity of the fungal nested PCR assay was observed to be 10 CFU/ml. A 504 bp fungal band was observed at 10 6 dilution only (having the maximum fungal load) in Round I while in Round II of the nested PCR, bands were observed in all the dilutions, i.e., from 10 6 to 10 CFU/ml. All 71 proven cases of IFIs were processed by the nested PCR assay and restriction enzyme digestion was performed to identify the fungal pathogens. The genus-specific restriction enzymes used for the Candida species were BSeYI and Hpy188I while for the Aspergillus species Mn1I was used. Given in [Table - 2] and [Table - 3] are the fragment sizes obtained after digestion with the mentioned enzymes. The diagnostic sensitivity and specificity of the fungal PCR assay was 100% [Table - 4]. The concordance of our PCR RE assay was also found to be 100% [Table - 5]. Disscusion Clinical diagnosis of these infections is complicated by a lack of specific clinical signs and symptoms of the disease. Of 71 proven cases, 57 were Candida positive while the remaining 13 were Aspergillus positive. There was one sample which was positive for Trichosporon asahii. Among the Candida species isolated in our clinical specimens, 42% were Candida tropicalis, 31% were C. albicans, 16% Candida glabrata and 7% Candida species followed by 2% of C. krusei. Among the Aspergillus species, A. fumigatus (n=10) was the most predominant organism followed by A. flavus (n=3). In the present study, we targeted 18S rRNA since this region has conserved sequences in multiple copies while the others such as ITS 1/2, mitochondrial DNA are highly variable. The nested PCR was used to enhance the analytical sensitivity of the assay. The analytical sensitivity of the fungal nested PCR assay was observed to be 10 CFU/ml. A 504 bp fungal band was observed at 10 6 dilution (having the maximum fungal load) in Round I while in Round II, bands were observed in all dilutions, i.e., from 10 6 to 10 CFU/ml. This is an improvement from the methods reporting 100 CFU/ml. [4],[5] The primers were tested for their ability to identify their correct target organism. The primers were found to be highly specific. Thus no false positives were observed indicating a specificity of 100%. In our patient population, 49 were males while 22 were females. These patients were on antibiotics. The other risk factors that were observed were the presence of central venous catheter, use of steroids or other immunosuppressants, dialysis/renal support, use of total parenteral nutrition (TPN), pancreatitis and major surgery. These risk factors are analogous with those published earlier. [6],[7],[8] The diagnostic sensitivity and specificity of the fungal PCR assay was 100%. The concordance of our PCR RE assay was also found to be 100%. The sensitivity and specificity of our study were found to better than those reported in the literature. [4],[9],[10],[11] We have described a new, rapid, sensitive, reliable and cost-effective nested fungal PCR RE assay for the detection and identification of the Candida and Aspergillus species. Our nested PCR assay is able to detect DNA of both the species in blood, body fluids and tissue specimens. To increase the sensitivity of the PCR assay, obtaining samples before the institution of antifungal treatment and serial sampling are desirable. In conclusion, we have successfully standardized and validated a nested PCR for the rapid detection of Candida and Aspergillus species. Acknowledgments We thank the National Health and Education Society, P. D. Hinduja National Hospital and Medical Research Centre, for funding our study and the bacteriology technicians, Department of Microbiology, P. D. Hinduja National Hospital and Medical Research Centre, who helped us with the sample collection. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11097t2.jpg] [mb11097f1.jpg] [mb11097t4.jpg] [mb11097t3.jpg] [mb11097f2.jpg] [mb11097t5.jpg] [mb11097t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}