 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
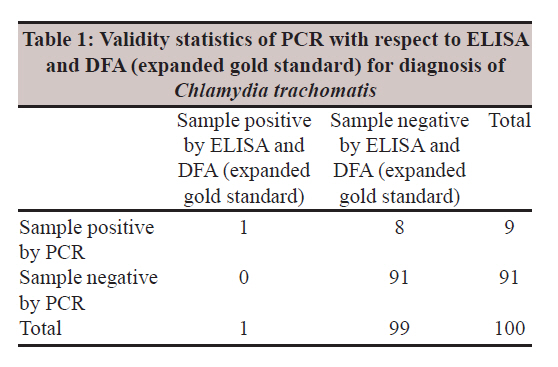
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 411-413 Brief Communication The role of a commercial enzyme immuno assay antigen detection system for diagnosis of C. trachomatis in genital swab samples A Mukherjee1, S Sood1, M Bala2, G Satpathy3, N Mahajan1, A Kapil1, VK Sharma4 1 Department of Microbiology, Dr. R.P. Centre for Ophthalmic Sciences, New Delhi, India Date of Submission: 05-Jul-2011 Code Number: mb11098 PMID: 22120804 Abstract In the present pilot study, endocervical and urethral swabs collected from 100 patients attending sexually transmitted disease (STD) clinics and regional centre for STD in two referral hospitals in New Delhi were analyzed by enzyme immune assay (EIA), polymerase chain reaction (PCR) and direct fluorescent antibody (DFA) for detection of C. trachomatis. It was found that EIA could detect a very low number of cases (3/100) as against DFA (11/100) and PCR (9/100). Thus, in spite of the widespread availability, lower cost and ease of performance of the enzyme-linked-immunosorbent serologic assay, the present study highlights the need to employ sophisticated diagnostic tools like DFA and PCR for detection of Chlamydia trachomatis in STD patients. Keywords: Direct fluorescent antibody, enzyme-linked-immunosorbent serologic assay, genital Chlamydia, polymerase chain reaction Introduction Chlamydia trachomatis accounts for 92 million cases annually on a global basis. [1] The diagnosis often poses serious problems as 70-80% of the women and 50% of the men have asymptomatic infections, leading to future complications, i.e. pelvic inflammatory disease causing ectopic pregnancy, infertility and other adverse health outcomes in women. [2],[3] In addition, Chlamydia infection appears to increase the risk of HIV transmission two to four times during sexual intercourse. Thus, while diagnosis of this silent disease is of utmost importance, it is technically challenging and requires sophisticated equipments and expertise. In India, reliable figures on incidence based on sensitive and specific techniques like nucleic acid amplification tests are lacking. [4] Hence, the present pilot study was conducted among symptomatic individuals for detection of C. trachomatis by three non-culture methods and the performance of the three methods was compared. Materials and Methods The sample size for the present study was calculated based on the results of previous published data in which the sensitivity of PCR was found to be 74.5%. [4] Taking the sensitivity of the reference test (DFA) to be 90%, [2] a sample size of 94 had 80% power and a two-sided confidence limit of 95% to detect this difference. Hence, a total of 100 patients presenting to the sexually transmitted diseases (STD) Outpatient Department (OPD) and the Regional STD Teaching, Training and Research Center located at two different referral hospitals in New Delhi were included in the study. Male patients presenting with burning micturition, dysuria, discharge per urethra and female patients complaining of cervical/vaginal discharge were included in the study. Three endocervical (female) and three urethral (male) swabs were collected from each patient. The first swab was used to prepare a bedside smear and was processed subsequently as per manufacturer′s instruction (Syva Microtrak, California, USA) for DFA. The second swab was used for antigen detection by a sandwich ELISA (Microtrak II, Behring, California, USA). The third swab was stored at -20°C for DNA extraction subsequently using the QIA amp DNA mini kit (Qiagen). The extracted DNA was stored at -20°C for PCR. The gene targeted was the common endogenous plasmid. The sequence of the primers was taken from a previously published study by Class et al. (1991) and are as follows. Forward primer 5′GGA CAA ATC GTA TCT CGG′3 Reverse primer 5′GAA ACC AAC TCT ACG CTG 3′ A 517-bps amplified product was to be obtained in positive control and samples. All reagents required for performing PCR were obtained from commercial source (Bangalore Genei, India) The necessary ethical clearance was obtained from the Ethics Sub-Committee of All India Institute of Medical Sciences, New Delhi. Results Of the 100 patients included in the study, 97 were females and 3 were males. The sex distribution is representative of the large percentage of female population attending the study centres. The age of the patients ranged from 15 to 50 years with an average of 29.87 years (S.D. = ±6.38). Out of the 100 swabs tested, 3 were positive for Chlamydia antigen by ELISA, 11 were positive (>10 Elementary Bodies/slide) by DFA and 9 were positive by PCR. Out of 9 samples positive by PCR, 8 were also positive by DFA (72.73% of DFA positive results). One PCR positive patient was negative for DFA. Discussion The enhanced syndromic approach advocates the use of laboratory techniques to confirm the clinical diagnosis in management of STI. In view of this recommendation, the present pilot study sought to evaluate three different techniques (ELISA, DFA and PCR) for detection of genital Chlamydia trachomatis infection. The main objective of the study was to compare the PCR against the expanded gold standard of ELISA and DFA. [5] We used the Microtrak II (Behring, California, USA) commercial EIA kit. This is a widely used and more recently developed commercial EIA for C. trachomatis. It has also shown to perform better for urogenital samples in comparison to some other widely used kits However, the low number of ELISA positive results prevented further statistical analysis. Traditionally, the detection of antigen by DFA has been accepted as a highly specific test because it involves direct visualisation of morphological structure under microscope. [6] In recent years, PCR has increasingly been accepted as a highly sensitive and specific test. In our study, we chose to target the common endogenous plasmid as it has more (7-10/cell) copy numbers, thus increasing sensitivity of the assay. Further, the chosen sequence was specifically checked for the absence of the 277 bp region whose deletion has been reported from variant strains of C. trachomatis (nvCT) from Sweden. However, DFA requires an experienced microscopist and a fluorescent microscope, while PCR requires trained personnel and sophisticated equipment, thereby limiting their use in peripheral centres. In this situation, ELISA was a logical alternative as it is less technically demanding and slightly less costly. Our initial objective was to describe the validity statistics of PCR with respect to expanded gold standard/defined reference standard (consistent positive results with two non-culture methods). However, the very low number of ELISA positivity (3/100) prevented further statistical analysis (low cell frequency <5 prevents meaningful statistical test in 2 × 2 table. However, taking ELISA and DFA as gold standard (expanded gold standard/defined reference standard), the one sample which was both ELISA and DFA positive was also positive for C. trachomatis by PCR. In that case, going by statistical analysis, the new test namely PCR is 100% (1/1) sensitive and 91.92% (91/99) specific [Table - 1]. Practically speaking, the results point to the low sensitivity and specificity of the ELISA used in the study. Since the number of DFA (11/100) and PCR (9/100) positive cases was much higher in number and there was a significant association between the two results, a conclusion regarding the performance of ELISA was made. Similar findings have been reported by other groups [7],[8] from different parts of the world and also from India. [9] The present study also suggests that ELISA may not work well even in symptomatic patients who shed reduced number of organisms as a result of prior antibiotic therapy. This aspect especially limits its use in tertiary referral centres where most patients receive a plethora of antibiotics before presenting to the hospitals. Thus, although ELISA-based methods are easier to perform, reasonably cheap and easily available, the findings of the present study show that the low detection rate of ELISA necessitates use of sophisticated tools like DFA and PCR for adequate case detection. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11098t1.jpg] |
| |||||||||
{kind=link}