 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
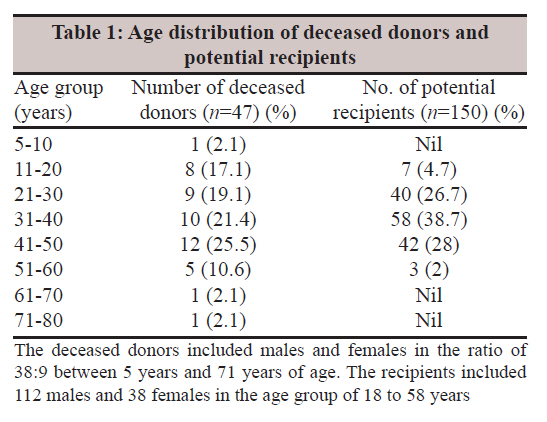
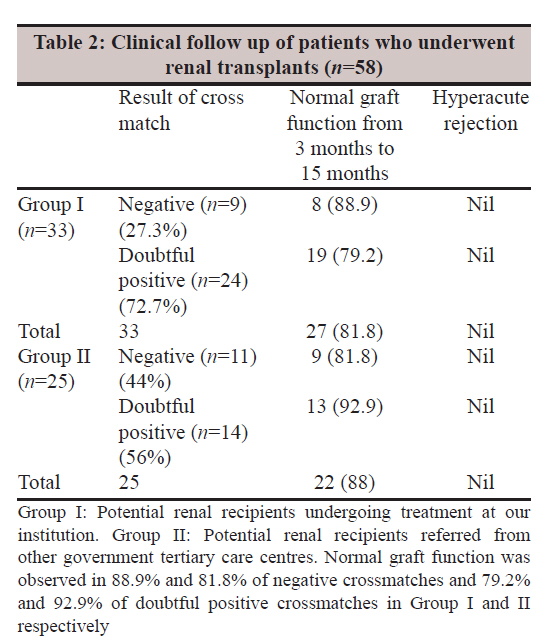
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 414-417 Brief Communication Complement-dependent lymphocytotoxicity crossmatch in deceased donor renal transplant: A single institutional experience R Deepa, P Balapriya, KG Venkatesh, T Sabeetha, J Sasikala, G Jayalakshmi Institute of Microbiology, Madras Medical College and Rajiv Gandhi Govt. General Hospital, Chennai 600 003, India Date of Submission: 11-May-2011 Code Number: mb11099 PMID: 22120805 Abstract Complement-dependent lymphocytotoxicity crossmatches (n=217) between 47 deceased donors and 150 potential renal recipients were retrospectively studied. A negative cross match was reported in 48 (22.1%), doubtful positive in 126 (58.1%), weakly positive in 32 (14.7%) and positive in 11 (5.1%). No autoantibodies were detected. Renal transplantation was performed in 35.5% of the potential recipients. There was no incidence of hyperacute rejection. The graft survival rate was 88% at 15 months of follow up. The study concludes that a negative pretransplant lympocytotoxicity crossmatch using the basic National Institute of Health technique eliminates hyperacute rejection, but carries drawbacks, which require modification and supplementation with more sensitive and specific assays. Keywords: Complement dependant lymphocytotoxicity, cross match, deceased donor renal transplant Introduction The Cadaver transplant programme in TamilNadu is a model programme in India and is noteworthy for its orientation toward poor patients in government hospitals. Vital organs from brain dead people, donated altruistically by their families, have provided a new life to several patients with organ failure. The most formidable barrier to making transplantation a routine medical treatment is the immune system. Cadaver donors are genotypically mismatches to the random recipient although there is a finite possibility of complete or partial phenotypic identity. [1] It is accepted that the role of antibodies is incontrovertible in hyperacute rejection although what fraction of acute rejection is humoral remains to be determined. [2] Graft acceptance between the cadaver donor and the selected recipient is promoted and immune rejection avoided through histocompatibility testing. The state of histocompatibility may be inferred from the absence of pre-formed antibodies in the recipient directed against donor HLA antigens. The simplest and fastest method to test for these antidonor antibodies is by the complement-dependent lymphocytotoxicity (CDC) crossmatch. [1] This study was done to analyse the results of histocompatibility crossmatches which were performed between deceased donor and potential renal recipients. Materials and Methods This retrospective study included 217 pretransplant CDC crossmatches which were performed from June 2009 to October 2010 between 47 deceased donors and 150 potential renal recipients placed in the waiting list of the deceased donor registry. All the samples tested negative for hepatitis B surface antigen, antibodies to HIV 1, 2 and HCV and were matched for blood groups. The CDC crossmatching was performed on recipient sera and peripheral blood lymphocytes of donor by the National Institute of Health Standard method. [1],[3],[4] Sample collection Blood (7.5 ml) was collected from each recipient, of which 5 ml was added to a test tube containing heparin. The remaining 2.5 ml was added to a clean test tube without anticoagulant. After centrifuge serum was separated. Separation of peripheral blood lymphocytes from donor and recipient Heparinised blood (3.5 ml) was gently mixed and diluted with 3 ml of phosphate buffer saline (PBS) to make a total volume of 6 ml.3 ml of lymphocyte separation medium (LSM), density 1.077 (Lymphoflot, Innotrain) was taken in a 15 ml graduated conical flask, overlaid gently with 5 ml of diluted heparinised blood and centrifuged at 2000 rpm for 30 min. The buffy coat was carefully pipetted out from the plasma-LSM interface and transferred to another test tube. The cells were resuspended in about 4 ml of PBS, mixed gently with a Pasteur pipette and centrifuged at 1000 rpm for 10 min. The supernatant is totally discarded and washing step repeated. After washing the buffy coat twice, the lymphocyte was suspended in 200-300 ml of PBS and counted in RBC square of a Neubauer counting chamber to attain a concentration of 2 × 10 6 /ml. The viability was checked by added by adding 1%Trypanblue. Viable cells were unstained while dead cells are stained. Complement dependant cytotoxicity crossmatch A drop of liquid paraffin was added to each well of a Terasaki tray. 1μl of recipient serum is added to each of three wells in the first column and to all the wells in the second column. This was followed by addition of 1 ml of negative control into the first three wells and 1μl of positive control to the last three wells in the third column. Auto crossmatch was performed by adding 1 m of recipient cells at the concentration of 2 × 10 6 /ml to the recipient sera in the first column.1ml donor cells at the concentration of 2 × 10 6 /ml was added to the second and third columns, the wells with the positive control to be dispensed last. The tray was incubated at 22°C for 30 min. The lyophilised rabbit complement was reconstituted with sterile distilled water prior to use.5 μl of complement was added to each of the wells and incubated for 60 min at 22°C. At the end of incubation, 5 μL of 4% eosin dye was added. After 5 min, 5 μl of formal saline was added to fix the reaction. The plate was read using an inverted microscope with a UV light source after 30 min. The percentage of dead cells in each well was noted and scored according to the International Histocompatibility workshop scoring system.0-10% cell death was interpreted as negative, 11-20% as doubtful positive, 21-50% as weakly positive, 51-80% as positive and 81-100% strong positive. Lysis of cells between recipient cells and recipient serum in the first column interpreted as positive for autoantibodies. Results Two hundred and seventeen consecutive crossmatches between 47 in-house and shared deceased donors and 150 prospective recipients were studied. The deceased donors included males and females in the ratio of 38:9 between 5 years and 71 years of age. The recipients included 112 males and 38 females in the age group of 18 to 58 years [Table - 1]. The number of recipients crossmatched against deceased donor lymphocytes ranged from a minimum of 1 to a maximum 10 on each occasion. Twelve potential recipients had a history of previous blood transfusion within the past 6 months. None had a previous transplant. Result of crossmatches Among a total of 217 crossmatches, a negative crossmatch was reported in 48(22.1%), doubtful positive in 126(58.1%), weakly positive in 32(14.7%) and positive in 11(5.1%). This included both single and repeat crossmatches. Although 217 crossmatches were performed, it was observed that the number of potential recipients was 150. The number of potential recipients for whom crossmatch was done only once was 108(72%). The remaining 109 crossmatches were repeat crossmatches for 42 recipients(28%). Thus, the sera of 26, 11, 2, 2 and 1 potential recipients were repeated twice, three, four times, five times and six times respectively for crossmatch with different deceased donors on different occasions. These samples which were repeated gave a negative cross match with different deceased donors subsequently. None of the potential recipients who had a weakly positive or positive crossmatch had history of previous blood transfusions or a previous transplant. None of the recipients was positive for autoantibodies in auto crossmatch. All the 12 potential recipients with history of blood transfusions had an initial negative crossmatch. Of the 150 prospective recipients, 92(61.3%) were under treatment in our institution (Group I), while the remaining 58 (38.7%) were referred from other Government tertiary care centres for crossmatching (Group II). Both groups underwent transplant in their respective institutions. Group I potential recipients (n=92) Thirty three (35.8%) cases underwent renal transplantation during this period. Twenty-seven (81.8%) of these renal recipients had a normal graft function ranging from 3 months to 15 months. One (3%) recipient developed graft artery thrombosis at 3 months and nephrectomy was done. Two cases expired due to sepsis at 1year (6.1%), two due to sepsis at 3 months (6.1%), one due to cerebral haemorrhage at 7 days (3%). There was no incidence of hyperacute rejection. The results of crossmatch and the clinical outcome are shown in [Table - 2]. The remaining 59 cases (64.1%) in the transplant registry are in the wait list for renal transplants. Group II potential recipients (n=58) Twenty-five cases (43.1%) underwent renal transplant in this group. Twenty-two cases (88%) of these renal recipients had normal graft function ranging from 3 months to 15 months. 3 (12%) cases died due to sepsis at 2 and 4 months. There was no hyperacute rejection. The results of crossmatch and clinical outcome are shown in [Table - 2]. The remaining 33 cases (56.9%) are wait listed in the renal transplant registry. Discussion The increasing awareness of the importance of deceased donor organ transplantation among the public is reflected in the statistics of the age distribution of the deceased donors ranging from 5 years to 80 years. A study on the influence of nonimmunologic factors on the outcome of extended criteria among deceased donor kidney transplants showed that donor age did not affect graft function or survival, or patient mortality. [5] The complement-dependent lymphocytoxicity with donor peripheral blood lymphocytes as the target is a standard pretransplant test. A positive cross match of more than 50% cell death by cytotoxicity clearly indicates the presence of antibodies to class I antigens. A weak positive crossmatch could result from an antibody specific for Class II or due to weak class I antibody. [4] The risk associated with sensitization against HLA class II in the absence of sensitization against HLA class I is negligible. [6] In our study, 14.7% crossmatches were weakly positive and 5.1% were positive. These recipients had a negative crossmatch subsequently with a different donor. To resolve the specificity of antibodies causing the weakly positive cross matches, cross matching with separated T and B lymphocytes or the more sensitive and specific assays such as solid phase immunoassays may be included in the protocol. [4] None of the recipients in the study group were positive for autoantibodies. These nonspecific antilymphocyte antibodies can be detected in the standard cytotoxicity method by performing the autocrossmatch. Auto antibodies can mask the presence of specific antidonor antibodies. [1] IgM autoreactive antibodies react with autologous as well as allogeneic lymphocytes in the CDC crossmatch test giving rise to false positive results and have been shown to be irrelevant to transplant outcome. Therefore, if autoantibodies are detected, performing an additional step during the crossmatch namely treatment of sera with dithiothreitol to eliminate IgM antibodies will ensure that transplantation is not denied on the basis of antibodies that will not affect transplant outcome. [7] Hyperacute rejection of the graft is the consequence of an inflammatory reaction due to the presence of undetected preformed antibodies occurring within the first 24 h of transplantation. [4] There was no incidence of hyperacute rejection in the renal recipients in our study. 35.5% of these recipients had a negative crossmatch and 65.5% had a doubtful positive crossmatch. A study by Ho et al., reported that screening and cross-matching the sera by complement-dependent cytotoxicity provides reliable results and optimizes the patient′s chances to receive a deceased-donor renal transplantation. [8] The graft survival rate of renal recipients in our study varied from 81% to 88% at 15 months in the two groups. The 2006 Organ Procurement and Transplantation Network/Scientific Registry of Transplant Recipients annual report indicates a graft survival rates for recipients of deceased donor non-expanded criteria donor kidneys of 91% at 1 year. [9] A study on cadaveric renal transplantation from India reported a patient survival rate at 1 year of 88.2% and graft survival rate of 73.5%. [10] To conclude, a negative pretransplant lympocytotoxicity crossmatch using the basic National Institute of Health technique eliminates hyperacute rejection, but carries drawbacks, which require modification and supplementation with more sensitive and specific assays. A comprehensive national protocol needs to be drawn to increase the accuracy of assessment of the level of risk to the transplanted organ, which shall be followed by institutions participating in the deceased donor transplant programme, for the purpose of maintaining uniform standards in testing. This will help to prolong graft and patient survival, prevent erroneous disqualification of a donor or recipient and to help effective utilisation of the organs of the deceased, which are generously donated by the kin in the midst of grief. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11099t2.jpg] [mb11099t1.jpg] |
| |||||||||
{kind=link}
{kind=link}