 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
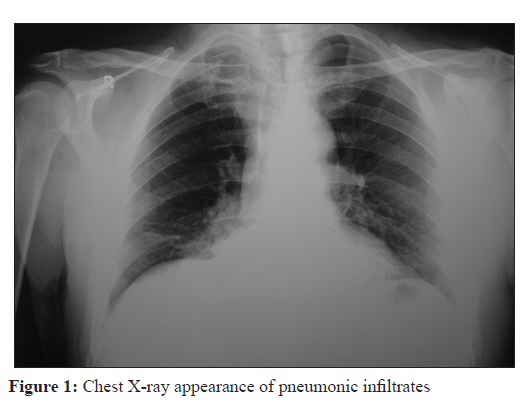
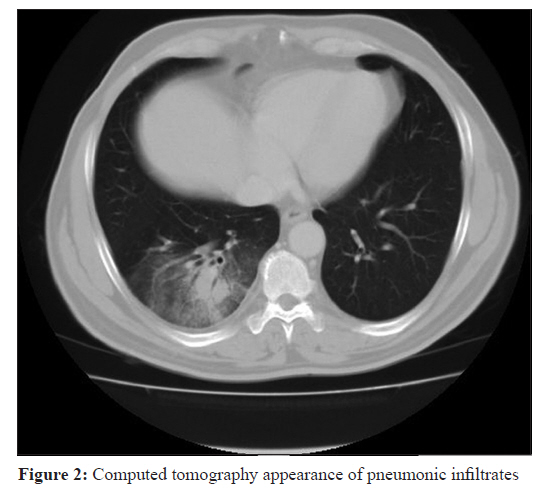
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 418-419 Case Report A Q fever case mimicking crimean-congo haemorrhagic fever O Karabay, HT Gozdas, G Ozturk, N Tuna, AC Utku Sakarya Training and Research Hospital, Department of Infectious Diseases and Clinical Microbiology, Turkey Date of Submission: 28-Apr-2011 Code Number: mb11100 PMID: 22120806 Abstract Coxiella burnetii is the bacterium that causes Q fever. Human infection is mainly transmitted from cattle, goats and sheep. The disease is usually self-limited. Pneumonia and hepatitis are the most common clinical manifestations. In this study, we present a case of Q fever from the western part of Turkey mimicking Crimean-Congo haemorrhagic fever (CCHF) in terms of clinical and laboratory findings. Keywords: Crimean-Congo haemorrhagic fever, clinical findings, laboratory findings, Q fever Introduction Q fever is a zoonosis caused by Coxiella burnetii. Main sources of transmission for human infection are cattle, goats and sheep. [1],[2] The disease is transmitted to humans through contaminated respiratory aerosols from urine, faeces, milk and birth products. [3] Incubation period may range from two weeks to one month. [4] Fever, fatigue, malaise, headache and myalgia are the most common symptoms. The disease is usually self-limited. Pneumonia and hepatitis are the most common clinical presentations. [5] Case Report A 59-year-old male was referred to our clinic with complaints of fever, severe headache, severe myalgia, fatigue and sweats beginning two days after a tick bite. It was learned that he had been in attendance during cattle-birth 15 days before. A tick bite was seen on his right elbow. Physical examination revealed the following: Fever: 38.3°C; pulse: 90/min; blood pressure: 110/70 mmHg; oxygen saturation: 94%; respiratory rate: 22/min. Spleen was palpable 2 cm below the left costal margin, firm and not tender. Laboratory findings were as follows: White blood cell count: 2.600 K/uL (N:4.6-10.2); haemoglobin: 12g/dl (N:12.2-18.1); haematocrit: 34.2% (N:37.7-53.7); platelet count: 85.000 K/uL (N:142.000-424.000); blood glucose: 89 mg/dl (N:74-106); urea: 40.3 mg/dl (N:16.6-48.5); creatinine: 1.1 mg/dl (N:0.70-1.20); alanine aminotransferase: 120 IU/L (N:1-41); aspartate aminotransferase: 87 IU/L (N:1-40); gama-glutamyltransferase: 234 IU/L (N:8-61); alkaline phosphatase: 267 IU/L (N:40-130); lactate dehydrogenase: 793 IU/L (N:240-480);, creatinine kinase: 80 IU/L (N:20-200); ferritin: 1384.82 ng/ml (N:21.81-274.66); C-reactive protein (CRP): 83 mg/l (N:0-5 mg/L); erythrocyte sedimentation rate: 85/h; prothrombin time: 11.6 sec (N:9.8-13.5); international normalized ratio (INR): 1.04 (N:0.85-1.3). Brucella tube agglutination test was negative. Chest X-ray [Figure - 1] and computed tomography scan [Figure - 2] showed pneumonic infiltrations in the lower lobe of right lung. Direct gram stain of the sputum was unremarkable; sputum culture and blood cultures showed no growth. Other laboratory findings were normal. He was admitted to inpatient clinic with presumptive diagnosis of Crimean-Congo haemorrhagic fever (CCHF) due to history of tick bite, bloody sputum and thrombocytopenia. Q fever was suspected in the differential diagnosis due to history of participation in cattle birth and symptoms of pneumonia. Considering CCHF as the presumptive diagnosis, ribavirin treatment was started. Serum samples for investigation of CCHF and Q fever were sent to reference laboratory. On the 4 th day of hospitalisation, the patient′s symptoms did not improve and thereafter CCHF ribonucleic acid (RNA) was reported negative. At this juncture, Q fever was thought of in the differential diagnosis. With this in mind, clarithromycin was started. On the 14 th day of admission, C. burnetii immunofluorescent antibody (IFA) immunoglobulin M (IgM) (phase 2) and IFA IgG (phase 2) were reported positive at 1/192 and 1/128 titer, respectively. The patient subsequently recovered completely over the next two weeks. Discussion CCHF is a viral disease caused by a member of Bunyaviridae family. It is transmitted through Hyalomma tick bites. [6] Fever, thrombocytopenia and easy bleeds may be observed during its course . Symptoms usually occur one to nine days after tick bite. [7],[8],[9] Our patient had fever, thrombocytopenia and bloody sputum. Hence, CCHF was thought as presumptive diagnosis. However, severe headache, participation in cattle birth, high CRP and erythrocyte sedimentation rate, pneumonic infiltrations on chest X-ray and computed tomography suggested atypical pneumonias in the differential diagnosis. Nonresponsiveness to ribavirin treatment, persistence of symptoms and the patient′s past history strongly suggested Q fever. Q fever is a zoonosis caused by C. burnetii. It is mainly transmitted from cattle, goats and sheep; however ticks may act as reservoir. The disease is usually self-limited. Pneumonia and hepatitis are the most common clinical manifestations. Symptoms usually occur two weeks to one month after transmission. [4],[10] Our patient had two risk factors for transmission of C. burnetii; one was tick bite and the other was attendance in cattle birth. Symptoms of pneumonia occurred only two days after tick bite and 15 days after participation in cattle birth. With this knowledge, C. burnetii was thought to be more likely transmitted from products of conception during attendance at cattle-birth. This case teaches us that Q fever should be considered in the differential diagnosis of patients with fever, cough, bloody sputum, leukopenia and thrombocytopenia. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11100f1.jpg] [mb11100f2.jpg] |
| |||||||||
{kind=link}
{kind=link}